The diagnosis of CVST is primarily made through imaging. However, not all medical centers have access to all types of imaging modalities. Previously, digital subtraction angiography (DSA) was considered the gold standard, but now less invasive methods like CT venography (CT-V) or MR venography (MR-V) are preferred [4].
These methods, particularly CT with or without contrast, are accessible and quick, allowing for a rapid diagnosis of cerebral venous thrombosis in the acute setting.
CT venography can be used as a reliable alternative to MR venography for confirming the diagnosis in patients with suspected CVST. [4, 5]
Imaging findings consist of two types of signs [6, 7]:
1. Direct signs:
- direct visualization of the thrombus on non-enhanced CT and conventional MRI sequences;
- visualization of the thrombus as a filling defect on CT/MR venography.
2. Indirect signs (occurring in 60% to 80% of cases) – parenchymal abnormalities seen on both CT and MRI:
- vasogenic edema;
- venous infarction, with or without associated hemorrhage;
- intraparenchymal hemorrhage;
- subdural hematoma, subarachnoid hemorrhage – rare manifestations;
- meningeal enhancement.
The location of the lesions is determined by the affected sinus [8]:
- superior sagittal sinus thrombosis – frontal and parietal lobes
- transverse sinus – temporal and occipital lobes
- vein of Labbe – temporal lobe
- deep veins and straight sinus – thalami, basal ganglia
Non-enhanced head CT (NECT) is the first intention method used for patients presenting with any new-onset neurological symptoms.
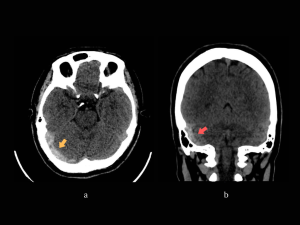
- the acute thrombus is identified as hyperdense material present in one or multiple dural sinuses – dense clot sign (Fig 3b, 11).
- on occasion, a hyperdense thrombosed cortical vein can be also seen – cord sign (Fig 8). [6,7]
CT venography (CTV) - can confirm the thrombosis as a filling defect.
* Arachnoid granulations can be visualized also as a filling defect. There are a few characteristics to differentiate them from thrombi – they typically have a round shape, their density/signal intensity is similar to CSF, and have characteristic locations [7] (Fig 12a)
The image acquisition CT-V protocol performed in our Emergency Department consists in:
Scan extent: C2 to vertex (head)/ aortic arch to the vertex (head and neck).
Contrast injection: 70-100 ml of non-ionic iodinated contrast with a debit of 3-4 ml/s.
Scan delay: a minimum of 45 seconds is necessary to achieve optimal enhancement of the dural sinuses.
Another option is to perform a CT-V study together with a CTA of the head and neck to evaluate both arterial and venous systems, especially in cases where the diagnosis is uncertain.

MRI is rarely used in an emergency but can be helpful when the diagnosis is uncertain. It can be used as a follow-up method to minimize radiation exposure.
Patent venous sinuses are seen as a flow void on conventional MRI. The thrombus can be seen in the following sequences [6, 8]:
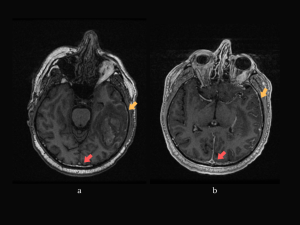
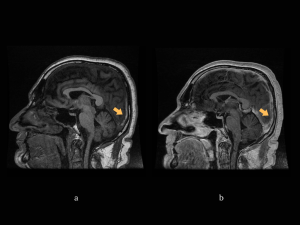
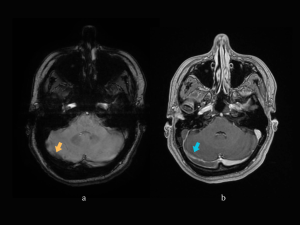
- T1 – hyper/isointense (Fig7a);
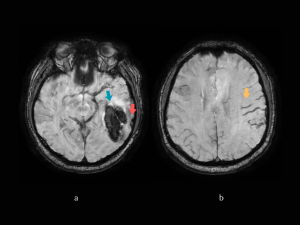
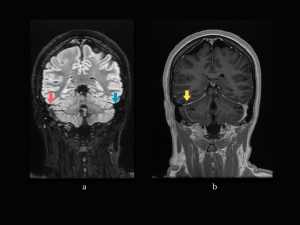
- T2/FLAIR – hypo/isointense in the acute stage (Fig 13a), and hyperintense later on;
- SWI (SWAN for GE scanners) - frank hypointensity (Fig 14a).
MR venography can be performed using the time-of-flight (TOF) or the phase contrast techniques without a contrast agent. The disadvantage of these techniques is the high susceptibility of flow-related artifacts. [8]
Gadolinium-enhanced MR venography uses the same principle as CT-V and it was proven to be superior to TOF MR venography. [8]
In the next section, we will describe four cases admitted to our emergency department with varying clinical presentations, as well as the results of each imaging method used.
CASE 1. 58-year-old man, presenting to the ED with severe mixed aphasia and repeated vomiting; history revealed headache that started a few days prior.
Neurologic examination: severe mixed aphasia, right temporal homonymous hemianopsia, no motor deficits.
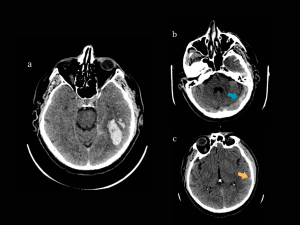
NECT: Left temporo-occipital hemorrhagic lesion, hyperdensity of the left transverse sinus, and hyperdense left inferior anastomotic vein (of Labbe). (Fig 3)
CT-V: extensive thrombosis on the following sinuses: left sigmoid and transverse, superior sagittal sinus in the posterior segment, and straight sinus. (Fig 4)
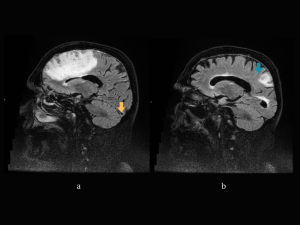
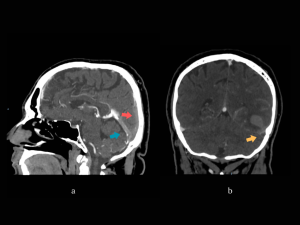
MRI and MR-V (3 days later): confirming the dural sinuses and vein of Labbe thrombosis, the hemorrhagic T-O lesion in the acute-subacute stage with mostly high intensity signal in T1, and low intensity in T2 and FLAIR and surrounding edema - venous hemorrhagic infarct. Also showing slight thickening and enhancement of the left hemisphere meninges. (Fig 5-7)
CASE 2. 23-year-old woman with a history of transverse myelitis and oral contraception use; recently experienced a few generalized seizures, last one the day before the presentation; also complaining of headache.
Neurologic examination: mixed aphasia, right-sided hemiplegia.
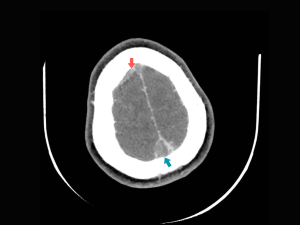
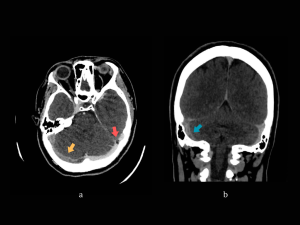
NECT: hyperdense superior sagittal sinus, left fronto-parietal and right parietal cortical veins, right transverse sinus; left hemisphere edema. (Fig 8)
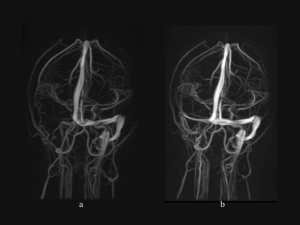
CT-V: confirming the thrombosis. (Fig 9)
MRI+MR-V: confirming the thrombosis and identifying a left fronto-parietal edematous lesion. (Fig 10)
A follow-up MRI was performed 3 months later showing complete remission of the lesions and recanalization of the thrombosed sinuses.
CASE 3. 25-year-old woman presents to the ED accusing intense right-sided headache that persisted a couple of days before admission; from the patient’s history we learn that she had a c-section 2 years ago.
Neurologic examination: normal.
NECT: hyperdense transverse sinus, sigmoid sinus and internal jugular vein on the right side. (Fig 11)
CT-V and MR-V: filling defect on the mentioned sinuses confirming the thrombosis. (Fig 12-15)
The patient was later diagnosed with hereditary thrombophilia (MTHFR A1298C mutation).
CASE 4. 71-year-old man with a history of chronic alcohol consumption is brought to the Emergency Department accusing left side motor weakness and confusion. The patient experienced multiple generalized seizures since admission.
Neurologic examination: left-sided hemiparesis.
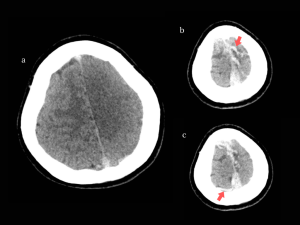
NECT: right frontal hypodense lesion with cortical involvement, with mass effect (compression of the right lateral ventricle) and subfalcine herniation. (Fig 16)
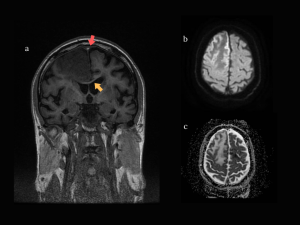
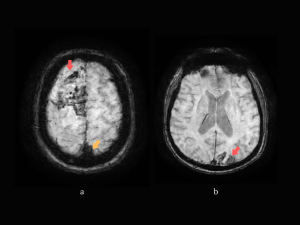
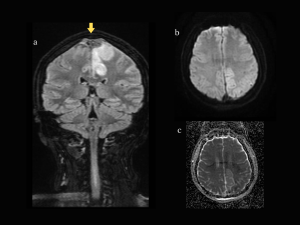
MRI + MR-V: right frontal lesion and another small left parietal lesion with similar characteristics: T1 hypointense signal, T2 and FLAIR hyperintense; peripheral restricted diffusion on DWI, without correspondent on ADC map. On SWAN sequence the lesions present areas of signal loss – consistent with hemorrhage. Thrombosis of the superior sagittal sinus, right transverse and sigmoid sinuses, and partial thrombosis of the left transverse and sigmoid sinuses. The lesions described are compatible with venous infarcts. (Fig 17-19)
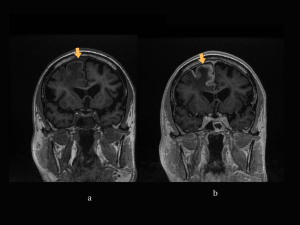
Follow-up MRI (10 days later): partial recanalization of the thrombosed sinuses, reduction of the mass effect determined by the right frontal lesion, which now appears with T1 cortical hyperintensity and gyral enhancement – a pattern of contrast enhancement seen in venous infarcts. (Fig 20)