Ovarian-Adnexal Reporting and Data System, Ultrasound (O-RADS US,)
O-RADS US applies to the ovaries, lesions involving (or suspected to involve) the ovaries and/or fallopian tubes, and paraovarian cysts, when the intent is to stratify risk of malignancy
Scenarios when O-RADS does not apply include (but are not limited to)
- Pelvic inflammatory disease, ectopic pregnancy, torsion of a normal ovary
- Lesions clearly identified as non-ovarian/non-tubal in origin (eg, an exophytic or broad ligament myoma)
- If the origin of a lesion is indeterminate, imaging options include CT and MR
- Ovary not seen or surgically absent - O-RADS US: Not applicable
- O-RADS US 0: Technically inadequate
- Ovarian visualization expected and required based on exam indication but not seen,eg: US follow-up of ovarian lesion previously seen or on another modality,High-risk patient (BRCA, etc.), screening US for ovarian cancer.
- Multiple or bilateral lesions• Each lesion should be separately characterized• Management driven by the lesion with the highest O-RADS score•Separate recommendations should be provided when management of one lesion is independent of the other
For risk stratification, the O-RADS US system uses five categories (O-RADS 1–5), from normal (1) to high risk of malignancy (5). An O-RADS US 0 (zero) category is used for an incomplete evaluation.
O-RADS 0 - is an incomplete evaluation due to technical factors such as bowel gas, large size of the lesion, location of the adnexa, or inability to tolerate endovaginal imaging.
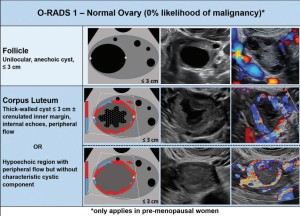
O-RADS 1-category relevant only in premenopausal patients, physiological findings such as the follicle and corpus luteum are included . To avoid confusion among patients, it is advisable for the ultrasound report to refer to these structures as a follicle and corpus luteum rather than using the term "cyst."
O-RADS 2, the almost certainly benign category (<1% risk of malignancy), comprises the majority of unilocular cysts less than 10 cm .
Simple Cysts:
- Unilocular cysts with smooth thin walls, acoustic enhancement, and anechoic internal content.
- Widely considered benign with strong literature support.
- Large studies indicate minimal malignancy risk, especially in premenopausal women.
Classic Benign Lesions:
- Emphasize using specific, classic benign features for accurate diagnosis.
- Avoid generic descriptors to prevent incorrect diagnoses and inappropriate management.
- Lesions with almost certain benign features are usually straightforward, but atypical cases may need further characterization by a US specialist or MRI.
- The goal is to reach a correct diagnosis, avoiding overtreatment
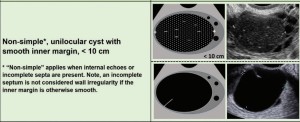
Nonsimple Unilocular Smooth Cysts: For unilocular cysts with smooth inner margins not fitting classic benign categories:
- Premenopausal (≤3 cm): No management needed.
- Premenopausal (>3 cm and <10 cm): Follow-up US in 8–12 weeks, preferably in the proliferative phase.
- If cyst persists or enlarges, consider referral to a US specialist or MRI study for further characterization.
- Postmenopausal (≤3 cm): Follow-up in 1 year is an option.
- Additional characterization recommended for all postmenopausal cysts, regardless of size, through US specialist or MRI study.
- Larger premenopausal cysts (>3 cm) and all postmenopausal nonsimple unilocular smooth cysts should be managed by a gynecologist
O-RADS 3 (1% to ,10% Risk of Malignancy)
- Over 90% are benign, reducing the need for gynecologic oncologist consultation.
O-RADS 4 (10% to ,50% Risk of Malignancy
- Consultation with gynecologic oncology or referral for management is warranted.
- Menopausal status, US specialist evaluation, MRI, and serum biomarkers (e.g., CA-125) may guide referrals to gynecologic oncologists.
O-RADS 5 (50%–100% Risk of Malignancy)
The system states that category 5 US findings (high-risk lesions) should be directly referred to a gynecologic oncologist for management.

The Ovarian-Adnexal Reporting and Data System (O-RADS) MRI risk score was developed by a multi-disciplinary international committee of experts as a codified scoring system for MRI evaluation of ovarian and adnexal lesions.
The O-RADS MRI risk stratification system provides a means for assigning probability of malignancy based on the composition of the lesion, the signal intensity characteristics, and the enhancement pattern of any solid tissue.
- Apply risk assessment to average-risk patients without acute symptoms for clinical management guidance.
- Dermoid or mature teratomas have low malignancy risk, assigned an O-RADS MRI risk score of 2.
- Some dermoids with minimal enhancing tissue maintain a score of 2; fat-containing lesions with substantial enhancing tissue may be scored 4 due to risk of malignancy.
- The final diagnosis can be reported with the O-RADS MRI score if classic imaging features are present.
- Dynamic contrast-enhanced MRI with time-intensity curves (TICs) is preferred for risk assessment.
- Inadequate studies merit an O-RADS MRI risk score of 0.
O-RADS MRI Score 0:
- Assigned when adnexal lesions are incompletely evaluated at MRI.
- Includes cases where portions of the lesion are not assessed or when technically inadequate MRI examinations occur (e.g., missing sequences, significant artifacts).
O-RADS MRI Score 1:
- Assigned when ovaries are normal.
- In premenopausal women, includes physiologic observations like follicles, hemorrhagic cysts, and corpus luteal cysts measuring 3 cm or less.
- In postmenopausal women, normal ovaries with very small residual follicles can be scored as 1.
- O-RADS MRI risk score does not apply to lesions identified as nonovarian or nonadnexal.
O-RADS MRI Score 2
- Almost certainly benign adnexal lesions.
- PPV for malignancy less than 0.5%.
- Includes unilocular cystic lesions without wall enhancement (proteinaceous, hemorrhagic, endometriotic fluid).
- Lesions with lipid content (mature teratomas or dermoids) are classified as O-RADS MRI 2.
- Lesions with homogenously hypointense signal on T2-weighted and high-b-value DWI scans are O-RADS MRI 2.
O-RADS MRI Score 3
- Adnexal lesions: Low risk for malignancy.
- PPV for malignancy approximately 5%.
- Includes unilocular cysts with smooth enhancing walls, hemorrhagic or proteinaceous fluid (no solid tissue).
- Multilocular cysts without solid tissue have very low malignancy risk.
- Endometriomas appearing multilocular are classified as O-RADS MRI 2.
- If enhancing solid tissue shows homogenously low signal intensity on T2/DWI scans, it's O-RADS MRI 2.
- If solid tissue doesn't fit the T2/DWI dark pattern, TIC enhancement characteristics dictate the score.
O-RADS MRI Score 4:
- Adnexal lesions: Intermediate risk for malignancy.
- PPV for malignancy approximately 50%.
- Lesions contain solid tissue exhibiting intermediate-risk TIC.
- Intermediate TIC shows a PPV of 46.6%.
- If DCE MRI not feasible, lesions with solid tissue enhancing ≤ myometrium at 30–40 seconds on non-DCE MRI are in this category.
O-RADS MRI Score 5
- Adnexal lesions: High risk for malignancy.
- PPV for malignancy approximately 50%.
- Lesions contain solid tissue exhibiting high-risk TIC.
- High-risk TIC shows a PPV of 85.6%.
- If DCE MRI not feasible, lesions with solid tissue enhancing > myometrium at 30–40 seconds on non-DCE MRI are in this category.