Participant inclusion and tumor progression
A total of 1177 participants were enrolled, 755/1177 (64.1%) who were self-assigned to AS and 422/1177 (35.9%) who were self-assigned to immediate surgery. Of the 755 AS subjects, 59/755 (7.8%) were excluded due to poor image quality. Additionally, 3/422 (0.7%) participants who underwent surgery had more than 2 US exams before their operation. Thus, 699 participants were included in our analysis. The baseline clinical characteristics of participants and US features of tumors are summarized in Table 1.
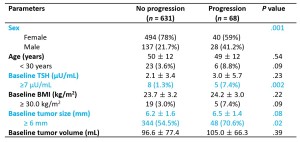
At the median period of 41.4 months (range, 4-60.2 months), 68/699 (10%) participants (mean age, 49 years ± 12 [SD]; 40 females, 28 males) showed tumor progression. Among these participants, 56/68 (82.4 %) were classified as having tumor enlargement, with a ≥3 mm increase observed in 18/68 (26.5%) participants, a ≥2 mm increase in at least two dimensions observed in 16/68 (23.5%) participants, and both ≥3 mm and ≥2 mm increase in two dimensions observed in 22/68 (32.4%) participants. Additionally, 3/68 (4.4%) participants developed extrathyroidal extension and 8/68 (11.8%) participants developed LNM. One participant (1/68, 1.5%) demonstrated an increase in tumor size (≥3 mm) simultaneously with LNM.
Baseline Clinical characteristics and US features associated with PTMC progression
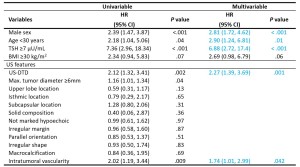
In the multivariable analysis, US-DTD (HR, 2.27; [95% CI: 1.39, 3.69]; P =.001) and presence of intratumoral vascularity (HR, 1.74 [95% CI: 1.01, 2.99]; P =.04) were independently associated with tumor progression along with male sex (HR, 2.82 [95% CI: 1.72, 4.62]; P <.001), age < 30 years (HR, 2.90 [95% CI: 1.24, 6.81]; P =.01), and TSH level ≥7 µU/mL (HR, 6.88 [95% CI: 2.72, 17.4]; P <.001) (Table 2).
Progression rates in subgroups stratified by US features
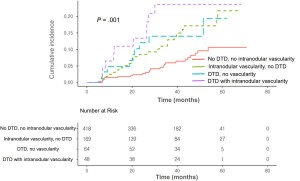
Using participants without US-DTD and intratumoral vascularity as reference, the tumor progression HR was 3.5 for participants with US-DTD and intratumoral vascularity (95% CI: 1.32, 9.23), 2.2 for participants with intumoral vascularity without US-DTD (95% CI: 0.97, 5.14), and 2.2 for participants with US-DTD without intratumoral vascularity (95% CI: 1.26, 3.89). These US-feature-based subgroups accurately stratified risk of tumor progression (log rank, P =.001, Figure 1).
Clinical characteristics and US features associated with tumor progression
Tumor enlargement of ≥3 mm were associated with male sex (HR, 3.25 [95% CI: 1.72, 6.15]; P <.001), age<30 years (HR, 3.48 [95% CI: 1.21, 10.0]; P = .02), US-DTD (HR, 2.69 [95% CI: 1.43, 5.07]; P = .002), and TSH ≥ 7 µU/mL (HR, 10.66 [95% CI: 3.72, 30.55]; P <.001), (Table 3).
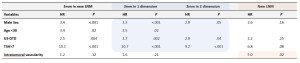
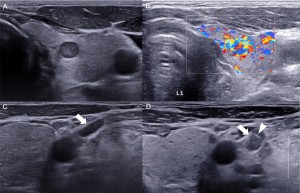
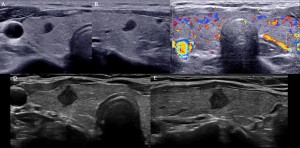
Male sex (HR, 1.95 [95% CI: 0.99, 3.84]; P = .05), US-DTD (HR, 2.0 [95% CI: 1.05, 3.8]; P <= .04), and TSH ≥ 7 µU/mL (HR, 9.16 [95% CI: 2.79, 30.07]; P <.001) also showed an association with tumor enlargement ≥2 mm in at least two dimensions. For new LNM, only intratumoral vascularity showed independent association (HR, 5.01 [95% CI, 1.29, 19.43]; P =.02). Representative US images at baseline and follow-up from a participant who developed LNM and a participant with tumor enlargement are shown in Figures 2 and 3, respectively.