The first step in the radiological approach, when faced with an air lesion, is to make a radiologic distinction between a true lung cyst and a cyst-like lesion. We must assess their size, wall thickness, number, location, distribution, and associated radiologic findings, to distinguish between true lung cysts and cyst-like lesions.
STEP 1: Are there true lung cysts?
A true lung cyst is a round parenchymal lucency with a well-defined interface with normal lung parenchyma, usually with a thin-walled (<2 mm) and without associated pulmonary emphysema.
Single cysts in a localized area of the lung should be distinguished from a cavity, pneumatocele, or bullae. Multiple cysts diffusely distributed should be differentiated from emphysema, honeycombing and cystic bronchiectasis.
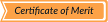
- CAVITY: focal lucency or low-attenuated area within pulmonary consolidation, nodule or mass, with a variable relatively thick and irregular wall thickness.
 Fig 3: Cavity
Fig 3: Cavity Fig 4: Cavity example. Pulmonary hidatid infection
Fig 4: Cavity example. Pulmonary hidatid infection Fig 5: Cavity example. Thoracic endometriosis
Fig 5: Cavity example. Thoracic endometriosis - PULMONARY BULLAE: focal lucency of more than 1 cm in size with a thin and imperceptible wall (not greater than 1 mm), usually accompanied by paraseptal and centrilobular emphysema. They are often subpleural in location and typically larger in the apices. In some cases, bullae can be very large and result in compression of adjacent lung tissue simulating pneumothorax.
 Fig 6: Pulmonary bullae
Fig 6: Pulmonary bullae Fig 7: Giant pulmonary bullae
Fig 7: Giant pulmonary bullae - PNEUMATOCELE: thin-walled round lucency lesions in the lung parenchyma accompanied by adjacent consolidation or ground-glass opacity, caused by pneumonia, trauma or aspiration of hydrocarbon fluid. They may progressively increase in size over the following days or weeks, and then resolve after weeks or months.
 Fig 8: Pneumatocele
Fig 8: Pneumatocele Fig 9: Pneumatocele example. Postneumonic pneumatocele
Fig 9: Pneumatocele example. Postneumonic pneumatocele - CENTRILOBULAR EMPHYSEMA: pulmonary emphysema is classified into three subtypes: centrilobular, paraseptal and panlobular. Centroacinar emphysema is defined by the presence of destroyed centrilobular alveolar walls and enlarged respiratory bronchioles and associated alveoli. It has a predilection for the upper lobes.
 Fig 10: Centrilobular emphysema
Fig 10: Centrilobular emphysema - HONEYCOMBING: honeycombing sign represents multiple rows of numerous thick fibrous well-defined walls cystic airspaces indicative of destroyed and fibrotic late stages of several lung diseases. It predominates in subpleural regions of the lower lobes. It is usually accompanied by other features of lung fibrosis, such as reticulation and traction bronchiectasis.
 Fig 11: Honeycombing
Fig 11: Honeycombing - CYSTIC BRONCHIECTASIS: bronchiectasis are an irreversible, localized, or diffuse bronchial dilatation, resulting from chronic infection, proximal airway obstruction or congenital bronchial abnormalities. Radiologic findings such as branching patterns, associated bronchial wall thickening, centrilobular densities and air-trapping differentiate bronchiectasis from simple cysts.
 Fig 12: Cystic bronchiectasis
Fig 12: Cystic bronchiectasis
Once we have ruled out a cystic-like lesion, we continue with the diagram.
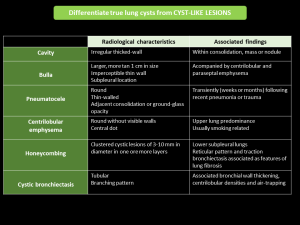
STEP 2: Solitary or multiple-localized or multiple-diffuse cysts?
- SOLITARY CYSTS:
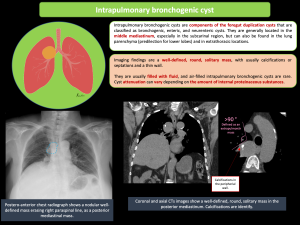
CONGENITAL CYSTIC LUNG DISEASE: BRONCHOGENIC CYST
Intrapulmonary bronchogenic cysts are components of the foregut duplication cysts that are classified as bronchogenic, enteric, and neurenteric cysts. They are generally located in the middle mediastinum, especially in the subcarinal region, but can also be found in the lung parenchyma (predilection for lower lobes) and in extrathoracic locations.
Imaging findings are a well-defined, round, solitary mass, with usually calcifications or septations and a thin wall.
They are usually filled with fluid, and air-filled intrapulmonary bronchogenic cysts are rare. Cyst attenuation can vary depending on the amount of internal proteinaceous substances.
- MULTIPLE/LOCALIZED CYSTS
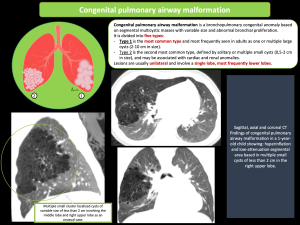
CONGENITAL CYSTIC LUNG DISEASE: CONGENITAL PULMONARY AIRWAY MALFORMATION
Congenital pulmonary airway malformation is a bronchopulmonary congenital anomaly based on segmental multicystic masses with variable size and abnormal bronchial proliferation. It is divided into five types:
- Type 1 is the most common type and most frequently seen in adults as one or multiple large cysts (2-10 cm in size).
- Type 2 is the second most common type, defined by solitary or multiple small cysts (0,5-2 cm in size), and may be associated with cardiac and renal anomalies.
Lesions are usually unilateral and involve a single lobe, most frequently lower lobes.
- MULTIPLE/DIFFUSE CYSTS
STEP 3: Associated with nodules?
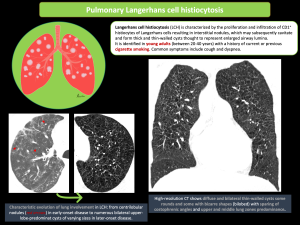
PULMONARY LANGERHANS CELL HISTIOCYTOSIS
Langerhans cell histiocytosis is characterized by the proliferation and infiltration of CD1 histiocytes of Langerhans cells resulting in interstitial nodules, which may subsequently cavitate and form thick and thin-walled cysts thought to represent enlarged airway lumina.
It is identified in young adults (between 20-40 years) with a history of current or previous cigarette smoking. Common symptoms include cough and dyspnea.
Radiologically, it is defined by small centrilobular nodules (smaller than 5 mm in diameter with irregular margins) in early disease and cystic airspaces thin-walled (< 10 mm in diameter), usually round or bizarre shapes in later disease, with an upper or middle lung zones predominance with costophrenic angles spared.
CYSTIC LUNG METASTASIS
Cystic lung metastasis are most frequently seen in patients with angiosarcoma or squamous cell carcinoma, mainly in the head and neck.
Radiologically, multiple solid nodules and multiple thin-walled cysts are often mixed with hemorrhagic change. There is a large variability in the wall thickness, air-fluid levels, and vessels or bronchi penetrating the cysts. If cystic lung lesions are seen in patients with a known malignancy, metastatic disease should be suspected, and tissue diagnosis be needed to establish the diagnosis.
PULMONARY AMYLOIDOSIS
Pulmonary amyloidosis is relatively rare, it can occur accompanied by Sjogren´s syndrome and mucosa-associated lymphoid tissue lymphoma.
Lung cysts are commonly numerous (>10), usually in peribronchovascular or subpleural regions, and frequently associated with nodular lesions that are often calcified. Cysts tend to be multiple, round or lobulated, small to moderate in size, and thin-walled. Other associated findings: interlobular septal thickening, honeycombing, ground-glass opacity, circumferential thickening of the tracheal wall, and lymphadenopathy.
STEP 3: Associated with ground-glass opacities?
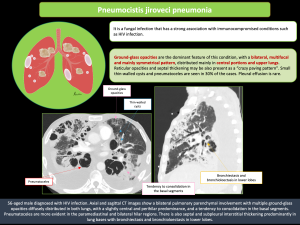
PNEUMOCISTIS JIROVECI PNEUMONIA
It is a fungal infection that has a strong association with immunocompromised conditions, such as HIV infection.
Ground-glass opacities are the dominant feature of this condition, with a bilateral, multifocal and mainly symmetrical pattern, distributed mainly in central portions and upper lungs. Reticular opacities and septal thickening may be also present as a “crazy paving pattern”. Small thin-walled cysts and pneumatoceles are seen in 30% of the cases.
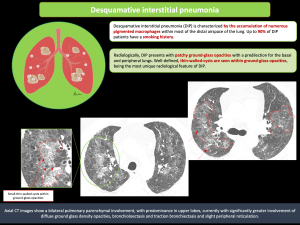
DESQUAMATIVE INTERSTITIAL PNEUMONIA
It is characterized by the accumulation of numerous pigmented macrophages. Up to 90% of patients have a smoking history.
It presents with well-defined thin-walled-cysts within ground-glass opacities, with a predilection for the basal and peripheral lungs.
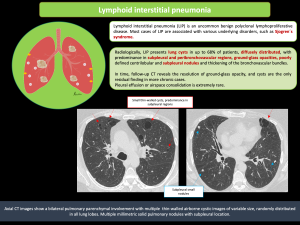
LYMPHOID INTERSTITIAL PNEUMONIA
It is an uncommon benign polyclonal lymphoproliferative disease, mostly associated with Sjogren´s syndrome.
It consists of extensive bilateral ground-glass opacities and poorly defined centrilobular nodules; other common findings include subpleural nodules, thickening of the bronchovascular bundles, thin-walled cystic airspaces and patchy ground-glass opacity.
STEP 3: No others radiologic findings associated?
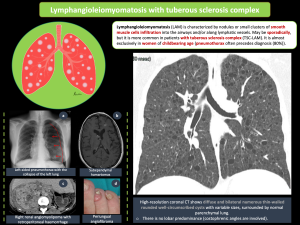
LYMPHANGIOLEIOMYOMATOSIS
Lymphangioleiomyomatosis is characterized by nodules or small clusters of smooth muscle cells infiltration into the airways and/or along lymphatic vessels. May be sporadically, but it is more common in patients with tuberous sclerosis complex. It is almost exclusively in women of childbearing age. Pneumothorax often precedes diagnosis.
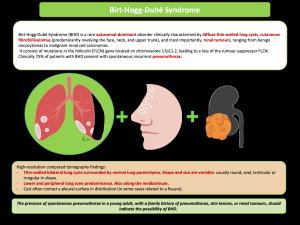
BIRT-HOGG-DUBÉ SYNDROME
It is a rare autosomal-dominant disorder clinically characterized by diffuse thin-walled lung cysts, with lower and peripheral lung zone predominance, cutaneous and renal tumours. 75% of patients present spontaneous recurrent pneumothorax.