Localization of Retroperitoneal Tumors
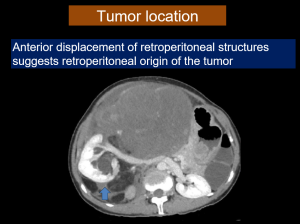
Before examining the specific imaging features of retroperitoneal masses, the radiologist must first confirm whether the mass is arising from the retroperitoneal soft tissue as opposed to the peritoneum or an organ that resides in the retroperitoneum. The clinical importance of making this distinction is that frequently, fat containing tumors arising from the retroperitoneal soft tissue turn out to be malignant while similar tumors arising from retroperitoneal organs like kidneys often turn out to be benign [8].
1. Tumor location: displacement of retroperitoneal organs or vascular structures often suggest that a mass is retroperitoneal in location.
2. Exclude organ of origin:
The following signs help in localizing the lesion to the retroperitoneum:
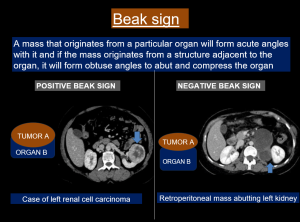
- Beak or claw sign
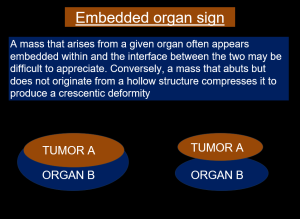
- Embedded organ sign
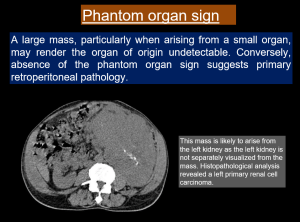
- Phatom organ sign
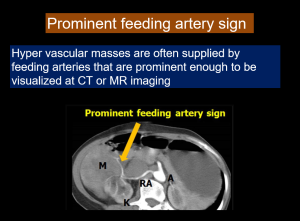
- Prominent feeding artery
Differential diagnosis of primary retroperitoneal masses
SOLID RETROPERITONEAL MASSES
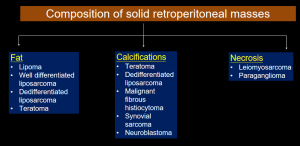
Solid primary retroperitoneal masses can be broadly divided into neoplastic and non neoplastic categories.
Solid neoplastic mass lesions:
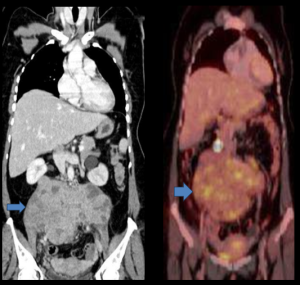
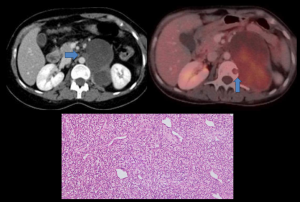
1. LYMPHOMA
- Lymphoma is the most common retroperitoneal malignancy, accounting for ~ 33% of all primary retroperitoneal masses.
- They typically present as para aortic masses with homogeneous attenuation and show mild homogeneous post contrast enhancement [4].
- They often appear as mantle like masses between the aorta and IVC, encasing the structures without compression. The aorta and IVC can be anteriorly displaced by the mass producing the classic "Floating aorta sign" or the "CT angiogram sign".
Take home point: Homogeneously enhancing retroperitoneal lesions with the "floating aorta" sign should raise the suspicion of retroperitoneal lymphoma.
2. SARCOMAS
Sarcomas are rare neoplasms of mesenchymal origin which account for about 15% of primary retroperitoneal tumors.
RETROPERITONEAL LIPOSARCOMA
- Liposarcoma is a malignant adipose tissue tumor which accounts for 15% of all soft tissue tumors. 10-20% of liposarcomas originate in the retroperitoneum [1].
- Histologically divided into 4 subtypes -
- Well differentiated - most common subtype with good prognosis, low metastatic potential, approximately 10% undergo dedifferentiation
- Myxoid - predominantly non fatty with a cystic appearance due to extracellular myxoid matrix. The presence of small amount of fat in lacy septa or nodular components is pathognomonic.
- Dedifferentiated - second most common subtype. Has the worst prognosis. Heterogeneous appearance with mixed solid and fatty components and the presence of calcifications is pathognomonic.
- Pleomorphic - least common subtype. Aggressive lesions with little or no macroscopic fat.

Take home point: Heterogeneously enhancing retroperitoneal lesion with mixed solid and fatty components and calcifications should raise the suspicion of a dedifferentiated liposarcoma.
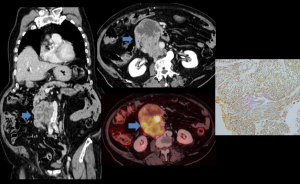
RETROPERITONEAL LEIOMYOSARCOMA
- Leiomyosarcoma is a malignant tumor of smooth muscle cells with a retroperitoneal location in 12-69% of cases.
- They manifest as large soft tissue masses with internal heterogeneity and heterogeneous enhancement usually secondary to necrosis and hemorrhage. Fat components and calcifications are usually absent.
- MRI: They normally show low to intermediate signal intensity on T1W and intermediate to high signal intensity on T2W images.

Take home point: A large non fat containing retroperitoneal mass with involvement of a contiguous vessel and varying internal necrosis should raise the possibility of a leiomyosarcoma.
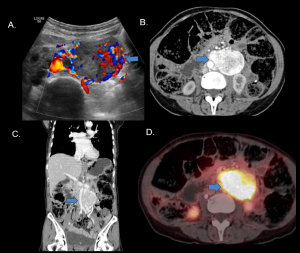
RETROPERITONEAL GIST
- Retroperitoneum is an exceptionally rare location for Gastrointestinal stromal tumors and account for less than 1% of cases [7].
- They arise from isolated Cajal's cells in the retroperitoneum.
- On contrast enhanced CT, they appear as heterogeneously enhancing lesions with no fat components or calcifications. Abdominopelvic MRI also helps to elicit the lack of fat within the lesion and the relationship with adjacent structures.
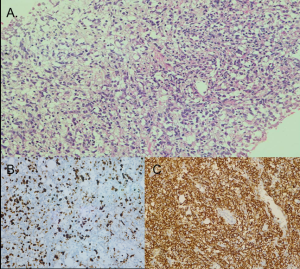
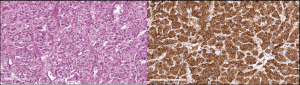
- Histopathological analysis with immunohistochemistry is required to establish the diagnosis. These mesenchymal tumors are c-KIT, CD-117, CD-34 and DOG-1 positive.
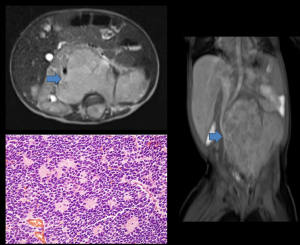
3. NEUROGENIC TUMORS
- Retroperitoneal neurogenic tumors account for about 10-20% of primary retroperitoneal tumors in adults.
- They are classified based on the tissue of origin:
- Nerve sheath: Schwannoma, neurofibroma, malignant peripheral nerve sheath tumor
- Ganglion cells: Ganglioneuroma, ganglioneuroblastoma, neuroblastoma
- Paraganglionic cells: Paraganglioma
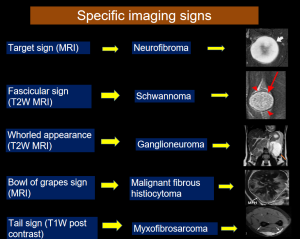
Take home points:
- Extra adrenal retroperitoneal paragangliomas are hypervascular intense arterial phase enhancing lesions most commonly originating from the organ of Zuckerkandl at the origin of inferior mesenteric artery. Strongly enhancing retroperitoneal masses in a hypertensive patient should raise the suspicion of a functioning paraganglioma.
- Malignant peripheral nerve sheath tumors account for 10% of all soft tissue sarcomas. Distinguishing features from neurofibroma include large tumor size, peripheral enhancement, perilesional edema, ill defined borders and increased FDG uptake.
- Retroperitoneal neuroblastomas arise from the paraspinal sympathetic chain in the retroperitoneum. They frequently cross the midline and appear as heterogeneously enhancing lesions which often show areas of necrosis and hemorrhage.
4. GERM CELL, SEX CORD AND STROMAL TUMORS
- Primary extra gonadal germ cell tumors are rare, accounting for 1 - 2.5% of germ cell tumors. A gonadal primary must be excluded first as majority of retroperitoneal germ cell tumors represent metastases.
- Teratomas account for approximately 11% of primary retroperitoneal tumors and is the third most common retroperitoneal tumor in children after neuroblastoma and Wilm's tumor. Teratomas are of two types - mature (dermoid cyst) and immature.
Solid non neoplastic mass lesions
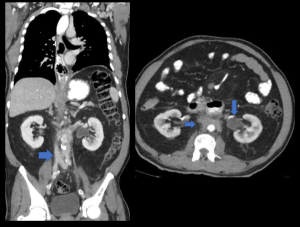
RETROPERITONEAL FIBROSIS
- Retroperitoneal fibrosis is a rare collagen vascular disease that is most common in men of fourth to sixth decades.
- Retroperitoneal fibrosis can be idiopathic or secondary to other etiologies like malignancy, medications or infections.
- On unenhanced plain CT, retroperitoneal fibrosis appears as a soft tissue attenuation mass surrounding aorta, inferior vena cava and psoas major with obliteration of fat planes. Retroperitoneal fibrosis displaces the ureters medially.
- In the acute stage of the disease, intense post contrast enhancement can be observed in CT and MRI. During the later stages, the lesion shows mild or even no contrast enhancement.
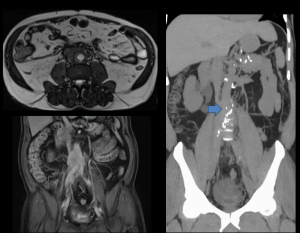
Take home point: Displacement of aorta, invasion of adjacent soft tissue structures and bone, peripheral lobulation and variable contrast enhancement can help distinguish malignant from benign retroperitoneal fibrosis.
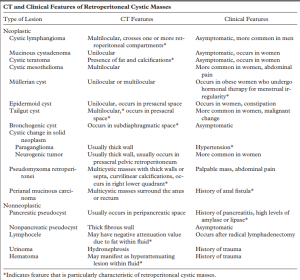
CYSTIC RETROPERITONEAL MASSES
Common cystic retroperitoneal masses, their classification, clinical and imaging features have been enlisted in the table below.
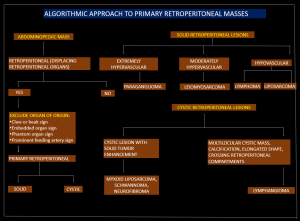
ALGORITHMIC APPROACH TO PRIMARY RETROPERITONEAL MASSES
Given below is a step by step algorithmic approach which could be used to confirm the retroperitoneal origin of a mass lesion and arrive at an appropriate diagnosis after excluding differentials.
STEP 1: Confirm the retroperitoneal origin of tumor based on the imaging signs discussed above.
STEP 2: Based on the imaging appearance, classify the lesion broadly as solid or cystic.
STEP 3: Classify the lesion based on location, vascularity, composition and specific imaging features.