Malformations of the upper urinary tract define a wide spectrum of disorders that occur in 3%-10% of the population, accounting for 50% of all congenital abnormalities. They are frequently associated with other congenital anomalies.
To make it simple, we’ll directly dive into the subject and divide these malformations into anomalies of renal form, including structural anomalies and fusion anomalies, anomalies of renal position, renal number, and anomalies of development of the urinary collecting system.
IMAGING APPROACH:
Antenatal screening ultrasonography allows the exploration of fetal kidneys and urinary bladder from the early second trimester and enables the diagnosis of some major congenital anomalies. This exploration consists of the assessment of the presence, location, and size of both kidneys, as well as their structures and echogenicity. Post-natal ultrasound can explore the same elements but in a more specific and accurate way. Contrast enhanced-US and voiding urosonography can be helpful in the evaluation of urethral abnormalities and the evaluation of vesicoureteral reflux. Cross-sectional imaging consists of computed tomography (CT) and magnetic resonance imaging (MRI).
Checklist:
- How many kidneys does the patient have?
- Are the kidneys in their normal position?
- How many collecting systems are there per kidney?
- Study the anatomy of each kidney: normal structure or not? Normal orientation? Distended excreting system? If this is the case, is there an obstruction to the urine excretion?
ANOMALIES OF RENAL FORM
- Structural anomalies are anatomical variants related to embryologic defects during the final stages of kidney development.
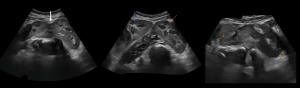
- Persistent fetal lobulation is due to incomplete fusion of the developing renal lobules and could be mistaken for renal scarring. It is seen as a smooth indentation of the renal outline in between pyramids as opposed to scarring where the indentation is not smooth and asymmetrical and overlies the renal pyramids.
 Fig 1: Kidney ultrasound showing persistent fetal lobulations.
Fig 1: Kidney ultrasound showing persistent fetal lobulations. - The Hypertrophied Column of Bertin is the extension of hypertrophied cortical tissue that separates the pyramids towards the central parenchyma. It is usually located in the mid portion of the left kidney and can be mistaken for renal mass. TIPS: it has continuity and the same characteristics as normal renal parenchyma.
 Fig 2: Ultrasound showing a hypertrophied column of Bertin (arrow)
Fig 2: Ultrasound showing a hypertrophied column of Bertin (arrow) - Dromedary Hump is a focal renal contour bulge caused by the splenic impression on the superolateral left kidney. Once again, it can be mistaken for a renal mass, but it has the same characteristics as renal parenchyma in any imaging modality.
- Persistent fetal lobulation is due to incomplete fusion of the developing renal lobules and could be mistaken for renal scarring. It is seen as a smooth indentation of the renal outline in between pyramids as opposed to scarring where the indentation is not smooth and asymmetrical and overlies the renal pyramids.
- Fusion anomalies occur during the cranial migration of the kidneys from the pelvis to the lumbar region.
- Horseshoe Kidney is formed by the fusion of two distinct functioning kidneys, one on each side of the midline. It may be a consequence of abnormal flexion or growth of the fetal spine and pelvic organs. This fusion traps the kidneys below the inferior mesenteric artery and is, therefore, responsible for a lower kidney location and an anteriorly facing pelvis. It mostly concerns the lower poles.
 Fig 3: Enhanced CT scan of a male patient showing a horse shoe kidneys. Note the fusion of the kidneys from their lower pole associated with renal malrotation. (a- axial, b-reconstructed to show the kidney fusion)
Fig 3: Enhanced CT scan of a male patient showing a horse shoe kidneys. Note the fusion of the kidneys from their lower pole associated with renal malrotation. (a- axial, b-reconstructed to show the kidney fusion) - Pancake kidney is characterized by an absence of a renal capsule and complete fusion of the superior, midline, and inferior poles of both kidneys in the pelvic cavity. Each kidney has its excretory system with two ureters that do not cross the midline and are not connected. There is a normal intersection of the ureters into the bladder. The blood supply can be anomalous in the number and origin of arteries. The US usually shows a large lobulated renal mass in the pelvic cavity without intervening septum.
- Horseshoe Kidney is formed by the fusion of two distinct functioning kidneys, one on each side of the midline. It may be a consequence of abnormal flexion or growth of the fetal spine and pelvic organs. This fusion traps the kidneys below the inferior mesenteric artery and is, therefore, responsible for a lower kidney location and an anteriorly facing pelvis. It mostly concerns the lower poles.
ANOMALIES OF RENAL POSITION
They occur because of defects in the cranial migration of the kidneys from the pelvis to the lumbar region.
- Renal Malrotation is defined as an abnormal position of the kidneys in relation to the hilum. Its prevalence is underestimated as it is usually asymptomatic. It consists of nonrotation or incomplete rotation, reverse rotation, hyper-rotating or excessive rotation, and sagittal rotation. Incomplete rotation and nonrotation are the most common. It exposes the patient to a higher risk of hydronephrosis, infection, and renal stones.
 Fig 4: Enhanced CT enterography showing an accidental finding of a malrotation of the right kidney
Fig 4: Enhanced CT enterography showing an accidental finding of a malrotation of the right kidney - Renal Ectopia: abnormal location of the kidneys, occurs when the kidney fails to ascend to the retroperitoneal renal fossa during embryonic development, making the pelvic position the most frequent one.
 Fig 12: Enhanced CT in sagittal view (a) and axial view (b) showing an ectopic left kidney in pelvic position with malrotation.
Fig 12: Enhanced CT in sagittal view (a) and axial view (b) showing an ectopic left kidney in pelvic position with malrotation. Fig 9: Axial and coronal MRI of an ectopic left kidney in a pelvic position associated with uterine agenesis.
Fig 9: Axial and coronal MRI of an ectopic left kidney in a pelvic position associated with uterine agenesis.
It can be simple when it is located on the same side as the ureter or crossed if the kidney is on the opposite side.
The position of the kidney in renal ectopia can be higher in the body as in subdiaphragmatic, and the renal ascension ends when the kidneys reach the adrenal glands.
When it comes to crossed ectopia, despite the ectopic renal position of the kidney, the ureter has a normal insertion in the bladder.

Crossed renal ectopia with fusion can be classified as inferior crossed fusion, S-shaped kidney, Lump Kidney, L-shaped kidney, Disc kidney, and superiorly crossed fused.
ANOMALIES OF RENAL NUMBER
They occur due to defects in the development of the ureteric bud or its interaction with the metanephric blastema.
- Renal agenesis: complete absence of one or both kidneys, it results from a lack of induction of the metanephric blastema by the ureteral bud. Bilateral agenesis is incompatible with life and associated with other congenital abnormalities. Unilateral agenesis is not uncommon and is often asymptomatic with compensatory contralateral hypertrophy.
 Fig 7: Axial abdominal MRI T2 weighted showing a unique left kidney (arrow), white empty renal space on the right side (dotted arrow). It was associated with uterine malformation bicornuate uterus (blue arrow)
Fig 7: Axial abdominal MRI T2 weighted showing a unique left kidney (arrow), white empty renal space on the right side (dotted arrow). It was associated with uterine malformation bicornuate uterus (blue arrow) Fig 8: Left renal agenesis with compensatory hypertrophic right kidney. (note an empty left renal space (arrow))
Fig 8: Left renal agenesis with compensatory hypertrophic right kidney. (note an empty left renal space (arrow)) - Supernumerary kidney: uncommon, is an additional accessory kidney that is seen on the left and caudal to native kidney. It is usually smaller in size with a reduced function. It is asymptomatic, although it may manifest as abdominal pain and a palpable mass.
ANOMALIES OF THE DEVELOPING URINARY COLLECTING SYSTEM
They are related to defects in the embryologic development of the ureteric bud starting during the 5th week of gestations.
- Duplex collecting system is one of the most common congenital tract abnormalities, characterized by an incomplete fusion of upper and lower pole moieties resulting in a variety of complete or incomplete duplications of the collecting system. Based on the degree of fusion, it can present bifid renal pelvis, partial ureteric duplication, incomplete ureteric duplication with ureters joining near or in the bladder wall (V-shaped ureter), and complete ureteric duplication with separate orifices. Double ureters follow the Weigert-Meyer rule, i.e., the upper moiety ureter inserts ectopically inferior and medial to the lower pole moiety ureter, with the upper moiety often ending in ureterocele with obstruction and lower pole moiety shows reflux. The inferior displacement of the opacified lower pole moiety realizes the drooping lily sign.
 Fig 10: Retrograde urethrocystography of a complete duplex collecting system on the right side following the Weigert-Meyer rule with vesicourethral reflux. Note the two collecting systems (arrows)
Fig 10: Retrograde urethrocystography of a complete duplex collecting system on the right side following the Weigert-Meyer rule with vesicourethral reflux. Note the two collecting systems (arrows) - Pyelocaliceal diverticulum, also called pyelogenic cyst, is a cystic dilatation of the renal pelvis or calyces, with narrow collecting system communication, lying in the renal parenchyma. When located in the calyces, it remains asymptomatic, but when it is pyelocaliceal, it is generally associated with stones and infection related to urinary stasis. The diagnosis is more accurate with intravenous urography, CT, or MR urography, which shows the contrast media filling the diverticulum during the excretory phase.
- Megacalycosis: enlargement of the renal calyces, the number of which may also be increased. Differentiating it from calyces enlargement due to obstructive causes can be challenging, at imaging, calyces appear enlarged with flattening of the renal pyramids with no or mild pelvic dilatation. Always think about excluding obstructive causes first.
- Ureteropelvic junction obstruction is defined as an obstruction of the normal flow of urine from the renal pelvis into the proximal ureter. It is the most common cause of postnatal hydronephrosis. At imaging, it appears as a dilated pelvis with an abrupt thinning of the collecting system at the ureteropelvic junction and calyceal dilatation.
- Megaureter is a broad term used to describe ureteral dilatation with or without associated pyelocaliceal dilatation. It can be considered normal if the ureter diameter is less than 0.5cm and the pathological is larger than 0.7cm. It can be either primary or secondary. Always look for an obstructive cause at first before concluding to a congenital megaureter. It is often associated with vesicoureteral reflux.
 Fig 11: megaureter: note the distension of the renal pelvis and the urethra.
Fig 11: megaureter: note the distension of the renal pelvis and the urethra.