1. INTRODUCTION AND ALGORITHMIC APPROACH
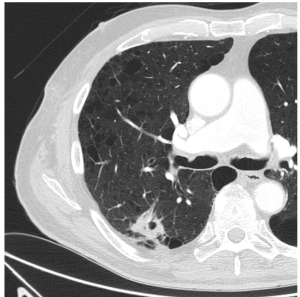
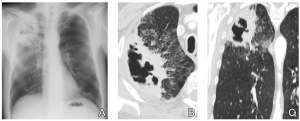
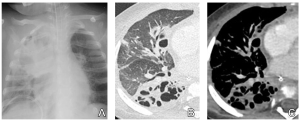
A CAVITY is defined by the Fleischner Society as "a gas-filled space, seen as a lucency or low-attenuation area, within pulmonary consolidation, a mass, or a nodule ... usually produced by the expulsion or drainage of a necrotic part of the lesion via the bronchial tree". Typically, it has a wall thickness greater than 4 mm (Fig. 1 and 2).
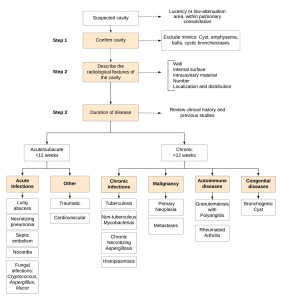
Due to the wide spectrum of clinical entities that may cause cavitary lung lesions, we should adopt a systematic approach that allows us to achieve an appropriate diagnostic approach (Fig. 3).
STEP 1. CONFIRM CAVITY
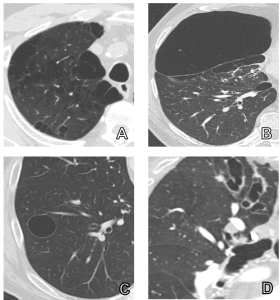
Distinguish it from other lesions with similar characteristics (mimics), such as (Fig. 4):
- Emphysema. Focal areas of low attenuation without visible walls.
- Bulla. Airspace measuring more than 1 cm, bounded by a thin wall (< 1 mm). Often accompanied by emphysematous changes.
- Cyst. A round circumscribed space, surrounded by an epithelial or fibrous wall of variable thickness, usually thin (< 2 mm), without associated pulmonary emphysema.
- Cystic bronchiectasis. Bronchial dilatation, with lack of bronchial narrowing and increased broncho-arterial ratio.
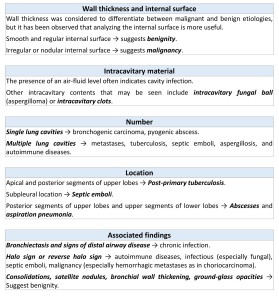
STEP 2: RADIOLOGICAL CHARACTERISTICS OF THE LESION (Fig. 5)
STEP 3: DURATION OF DISEASE AND CLINICAL CONTEXT
- Acute or subacute evolution (<12 weeks) suggests acute infectious, traumatic, or cardiovascular diseases.
- Chronic evolution (>12 weeks) suggests malignant, congenital, or chronic infectious etiology.
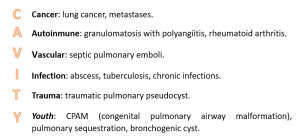
To remember the etiology of the cavitary lung lesions, we can use the mnemonic CAVITY (Fig. 6).
2. ACUTE/SUBACUTE CAVITARY LUNG LESIONS
2.1. INFECTION
2.1.1. Abscess
- Etiology: Polymicrobial, typically anaerobic bacteria and components of oral flora.
- Radiological findings (Fig. 7): Cavity with thick walls, irregular margins, and typically with an air-fluid level. Often unilateral and solitary. In patients with aspiration, the preferred location of these cavitary lesions is in the posterior segments of the upper lobes and upper segments of the lower lobes. It may be associated with pleural effusion, consolidations, tree-in-bud appearance, or empyema.
2.1.2. Necrotizing pneumonia
- Etiology: Bacterial causes include Staphylococcus aureus, Streptococcus pneumoniae, Klebsiella pneumoniae, Haemophilus influenzae, and Pseudomonas aeruginosa.
- Radiological findings (Fig. 8): Areas of consolidation containing areas of low attenuation that do not enhance, indicative of necrosis, which may form cavities. It may be associated with pleural effusion or empyema.
2.1.3. Septic pulmonary emboli
- Etiology: Staphylococcus, Fusobacterium necrophorum, Klebsiella pneumoniae…
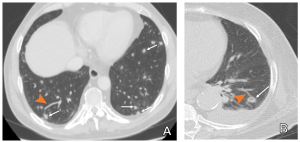
- Radiological findings (Fig. 9): Multiple peripheral well-defined nodules, of various size that can cavitate in up to 85% of patients. Typically seen in different stages of cavitation. The "feeding vessel sign" may be observed.
2.1.4. Nocardia
- Etiology: Nocardia asteroides.
- Radiological findings (Fig. 10): Nodules and consolidations, which can cavitate. A ground-glass pattern may surround them. Pleural effusion and bronchiectasis may also be present. The central nervous system is the most common extrapulmonary site affected, which can present as brain abscesses.

2.1.5. Cryptococcus
- Etiology: Cryptococcus neoformans.
- Radiological findings (Fig. 11): Single or multiple nodules that may coalesce. Masses, typically bilateral and predominantly peripheral, although random distribution can also occur. Cavitation is particularly common in immunocompromised patients.
2.1.6. Aspergillosis
Pulmonary aspergillosis is caused by the fungus Aspergillus (typically Aspergillus fumigatus), and can present in various forms:
- Allergic bronchopulmonary aspergillosis (ABPA)
- Airway invasive aspergillosis (or bronchopneumonic aspergillosis)
- Aspergilloma (saprophytic aspergillosis or non-invasive aspergillosis)
- Chronic necrotizing aspergillosis (semi-invasive aspergillosis)
- Angioinvasive aspergillosis
Cavitation can be found as an imaging finding in the last three.
Aspergilloma:
Infection of a preexisting cavity, usually caused by tuberculosis. It can also occur due to sarcoidosis, bullae, bronchiectasis, or cystic disease.
- Radiological findings (Fig. 12): A rounded mass of soft tissue density inside a cavity and separated from the cavity wall by an air space ("Monod sign"). This mass can change position when the patient moves.

Angioinvasive aspergillosis (Fig. 13):
The typical findings are nodules surrounded by a halo of ground-glass attenuation, corresponding to perinodular hemorrhagic infarctions (“halo sign”), although it is not pathognomonic. After effective treatment, nodules cavitate in up to 63% of cases, resulting in the “air crescent sign” due to tissue necrosis.
2.2. OTHER
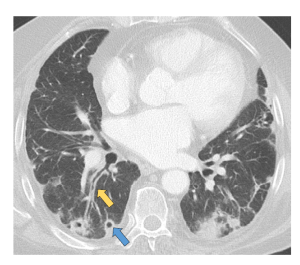
2.2.1. Pulmonary infarction (Fig. 14)
Infarctions secondary to pulmonary embolism appear as subpleural wedge-shaped opacifications, which can cavitate.

2.2.2. Trauma
It is uncommon for a traumatic lung injury to cavitate. If it does occur, the cavities typically have thin walls and may exhibit an air-fluid level if there is bleeding within the cavity. More frequently in the lower lobes.
3. CHRONIC CAVITARY LUNG LESIONS
3.1. INFECTION
3.1.1 Tuberculosis
Cavitation is characteristic of tuberculosis reactivation. More frequently in the apical and posterior segments of the upper lobes or in the upper segments of the lower lobe.
- Etiology: Mycobacterium tuberculosis.
- Radiological findings (Fig. 15): Consolidations, centrilobular nodules with a "tree-in-bud" appearance, fibrous tracts, volume loss, and cavitation. Multiple cavities with thick walls and irregular internal margins, which may become thin and smooth with treatment. Residual cavitary lesions may remain, which can be prone to bacterial superinfection or mycetoma formation.
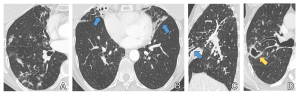
3.1.2. Non-tuberculous mycobacterias
Primarily caused by bacteria from the Mycobacterium avium complex (MAC).
Two groups of affected patients are distinguished:
The first group includes patients with immunosuppression or structural lung disease such as chronic obstructive pulmonary disease, silicosis, sequelae of tuberculosis, or cystic fibrosis.
- Radiological findings: Unlike tuberculosis reactivation, cavities caused by MAC are usually smaller and have thin walls, and the disease may progress more slowly. Tree-in-bud opacities or bronchiectasis may be associated.
A second group includes elderly women who present with chronic non-productive cough and weight loss.
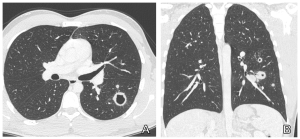
- Radiological findings (Fig. 16): Signs of chronic airways inflammation, bronchiectasis and tree-in-bud opacities, predominantly in the lingula and middle lobe. Severe cases may cavitate.
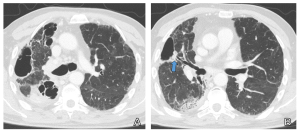
3.1.3. Chronic necrotizing aspergillosis
- Etiology: Aspergillus.
- Radiological findings (Fig. 17): Initially, a pulmonary opacity develops, which evolves into a central necrotic area ("air crescent sign"), and subsequently cavitation, which may harbor a mycetoma. Bronchopleural fistulas may be observed.
3.1.4. Histoplasmosis
- Etiology: Histoplasma capsulatum.
- Radiological findings (Fig. 18): Cavitation is less frequent than in tuberculosis, typically localized in the upper lobes. Cavities may be single or multiple, usually with thick walls. It may associate pulmonary fibrosis and calcified granulomas. The presence of numerous punctate calcifications in the spleen, liver, and mesenteric lymph nodes is suggestive of this entity.
3.2. MALIGNANCY
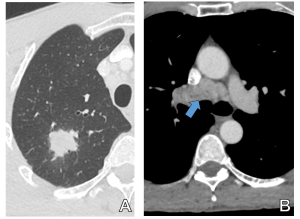
3.2.1. Primary lung neoplasm
Squamous cell carcinoma has a higher tendency to cavitate. The presence of cavitation is associated with a worse prognosis. Other primary lung tumors that may exhibit cavitation include lymphoma and Kaposi sarcoma. Cavitation is uncommon in small cell tumors.
- Radiological findings (Fig. 19): Single cavitated lesions are more frequent, with thick (≥15 mm), and irregular walls.

3.2.2. Pulmonary metastases
Lower tendency to cavitate than primary bronchogenic carcinoma. Metastases from head and neck squamous cell carcinomas have a higher tendency to cavitate.
- Radiological findings (Fig. 20): Multiple rounded lung masses of variable size, which may cavitate. The radiological appearance of the cavities varies, from thick and irregular to very smooth and thin.
3.2.3. Post-treatment cavitation
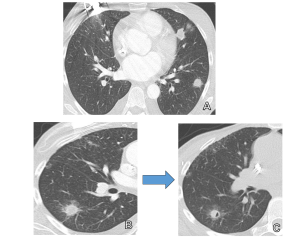
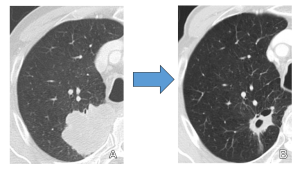
Central necrosis and cavitation of the tumor after chemotherapy treatment are signs of good response (Fig. 21). Post-radiotherapy cavitation of the tumor is also common.
3.3. AUTOIMMUNE DISEASES
3.3.1. Granulomatosis with Polyangiitis
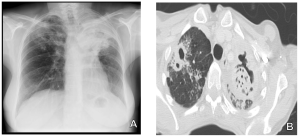
- Radiological findings (Fig. 22): Multiple bilateral nodules are detected in 40-70% of cases, with 25-50% of them cavitated, typically with thick walls. Granulomas in the kidneys and upper and lower respiratory tract may be associated, as well as signs of airways chronic inflammation.
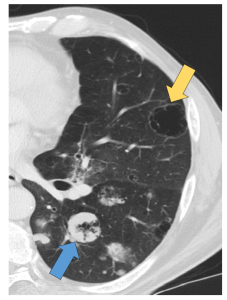
3.3.2. Rheumatoid arthritis
- Radiological findings (Fig. 23): Pulmonary rheumatoid nodules are present in up to 20% of cases. They appear as multiple well-defined nodules of variable size, which may develop central necrosis and cavitation. Other findings include signs of interstitial lung disease and pleural effusion.

3.3.3. Other autoimmune diseases
- Sarcoidosis: Hilar and mediastinal lymphadenopathy, with or without parenchymal involvement. It is rare for granulomas to cavitate.
- Less common: Ankylosing spondylitis, eosinophilic granulomatosis with polyangiitis, systemic lupus erythematosus.
3.4. CONGENITAL LESIONS
Congenital lesions presenting as pulmonary cavities include:
- Bronchogenic cyst
- Congenital pulmonary airway malformations
- Pulmonary sequestration.