Congress:
ECR25
Poster Number:
C-27591
Type:
Poster: EPOS Radiologist (educational)
Authorblock:
T. Cantarelli Rodrigues, I. R. B. Godoy, A. Fukunishi Yamada, A. Skaf; São Paulo/BR
Disclosures:
Tatiane Cantarelli Rodrigues:
Nothing to disclose
Ivan R. B. Godoy:
Nothing to disclose
André Fukunishi Yamada:
Nothing to disclose
Abdalla Skaf:
Nothing to disclose
Keywords:
Musculoskeletal joint, Conventional radiography, CT, MR, Surgery, Arthritides
INTRODUCTION
Definition and significance:
- DRUJ instability is a common, but often misdiagnosed, clinical condition.
- This instability often occurs in the setting of distal radius fractures, with incidence rates reported to be between 10-19%.
 Fig 1: (A) PA radiographic view of the distal forearm showing a Galeazzi fracture with a fracture of the distal radius (arrow) and associated disruption of the DRUJ (thick arrow). (B) Lateral radiographic view illustrate the degree of radial fracture displacement (arrow) and DRUJ instability, with dorsal dislocation of the distal ulna (chrevron).
Fig 1: (A) PA radiographic view of the distal forearm showing a Galeazzi fracture with a fracture of the distal radius (arrow) and associated disruption of the DRUJ (thick arrow). (B) Lateral radiographic view illustrate the degree of radial fracture displacement (arrow) and DRUJ instability, with dorsal dislocation of the distal ulna (chrevron). - A true lateral radiograph of the wrist with >50% uncovering of the ulna head points toward DRUJ instability as does a widened DRUJ interval >3 mm on a PA projection.

Fig 2: Radiographic images of a 31-year-old female patient with a distal radius fracture. (A, B): PA (A) and lateral (B) views showing an acute, comminuted distal radius fracture. (C, D): PA (C) and lateral (D) postoperative views demonstrating distal radius fracture fixation. Notably, there is an enlargement of DRUJ joint space (arrow) and dorsal dislocation of the distal ulna (chevron), indicative of DRUJ instability.
CLINICAL PRESENTATION AND SYMPTOMS
DRUJ instability is often overlooked in clinical and radiographic exams.
- Clinical Suspicion:
- History of wrist trauma
- Pain, limited motion with supination and pronation
- Patients may report feeling a "click" with forearm motion
- Physical Tests:
- Ballottement Test: Considered the most reliable physical examination test for DRUJ instability
 Fig 3: Ballottement test. The radius is grasped by the examiner and the distal ulna, fixed between the examiner's thumb and index. An increased anteroposterior displacement of the head of the ulna on the radius is considered a positive test.
Fig 3: Ballottement test. The radius is grasped by the examiner and the distal ulna, fixed between the examiner's thumb and index. An increased anteroposterior displacement of the head of the ulna on the radius is considered a positive test. - Radius Pull Test
- Clunk Test
- Extensor Carpi Ulnaris Test
- Press Test
- Ballottement Test: Considered the most reliable physical examination test for DRUJ instability
ANATOMY OF THE DRUJ
- Osseous Components:
- Radial Sigmoid Notch: Articulates with the ulnar head; contributes to joint stability.
- Ulnar Head: Includes the hub and seat, with the fovea and styloid serving as key attachment points for ligaments.
- Ulnar Styloid: Provides attachment for the peripheral TFCC.
- Intrinsic Stabilizers
- TFCC: Primary stabilizer of the DRUJ, restricting volar translation of the radius.
- Central Disk: Shock absorber, dissipating forces across the ulnar side of the wrist.
- Distal Radioulnar Ligaments: Major stabilizers, with dorsal and volar fibers that stabilize the joint in various wrist positions.
- Ulnocarpal Ligaments: Include the ulnolunate and ulnotriquetral ligaments, contributing to both DRUJ and ulnocarpal stability.
- Ulnomeniscal Homologue: Acts as a shock absorber, reinforcing the ulnar-sided joint capsule.
- Extensor Carpi Ulnaris Tendon and Subsheath: Provide minor stability to the DRUJ and prevent tendon subluxation.
- Extrinsic Stabilizers
- Pronator Quadratus: Stabilizes the DRUJ by tensing the capsule and preventing dorsal translation of the radius.
- Interosseous Membrane: Maintains longitudinal stability of the forearm, with the distal oblique bundle acting as a secondary stabilizer of the DRUJ.
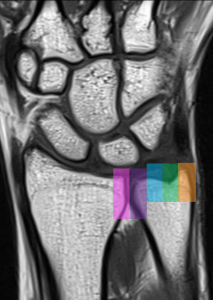
Fig 4: Coronal MR T1-weighted image of the wrist highlights the bony components of the DRUJ: the radial sigmoid notch (pink); the ulnar head, consisting of the hub (purple) and seat (blue); and the remaining distal ulna, including the fovea (green) and styloid (orange). The radial sigmoid notch aligns with the hub of the ulna, while the proximal surface of the triangular fibrocartilage complex (TFCC) interfaces with the ulnar seat.
IMAGING TECHNIQUES
- DRUJ instability can arise from the disruption of key ligamentous stabilizers as well as from disrupted articular geometry due to fractures.
- Defining the structures injured is crucial for management and diagnosis, as this guides the treatment.
- Radiographs, stress radiography, videofluoroscopy, and advanced imaging techniques improve the accuracy of diagnosis.
 Fig 5: (A) 3D reformatted CT scan in a patient with DRUJ instability.(B) Intraoperative wrist fluoroscopy during a DRUJ instability procedure following distal radial fracture fixation.
Fig 5: (A) 3D reformatted CT scan in a patient with DRUJ instability.(B) Intraoperative wrist fluoroscopy during a DRUJ instability procedure following distal radial fracture fixation.
Radiography
- Main imaging technique. Begin with radiographs to assess the surgical state, carpal alignment, and position of screws or anchors, and rule out bone alterations.
- Neutral views: PA, lateral.
- Additional Views: Oblique and with deviations.
- Limitations: Overlapping structures and soft tissue evaluation.
- Utility: Provides information in a neutral position, useful for assessing bone alignment and comparing with preoperative images.
Ultrasonography
- Effective for evaluating tendon sutures, vascular nerve injuries, and unstable injuries
- Limitations: TFCC, cartilage, and bone evaluation.
Computed Tomography (CT)
- Multiplanar Reconstructions
- Reduce Metal Artifacts: Metal reduction algorithms (MAR), Dual Energy CT
- Consider arthrographic CT when MRI is compromised by artifacts or for assessing bone anchors or other materials.
MRI
- MRI is preferred for postoperative assessment, especially for TFCC and ligament surgeries.
- Avoid: Wrist in a lateral position with supinated palm as it hinders evaluation of the ulnar side of the wrist and first carpal row.
- Reduce Metal Artifacts: Increase bandwidth, decrease echo time, use STIR, Dixon or specific protocols (MAVRIC/SEMAC).