Imaging has a role in the diagnosis, evaluation of the extent of disease, follow-up and surgical planning. The anatomic location, displacement of surrounding vessels and skull base involvement allow accurate diagnosis of the type of paraganglioma.
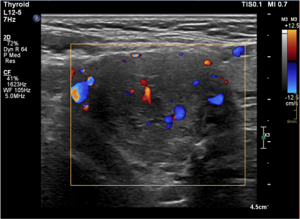
Ultrasound is commonly employed in the early stages of diagnosis of a neck mass, and in these cases a heterogeneously hypoechoic mass is typically observed (Figure 1), accompanied by pronounced internal vascularity on color Doppler.
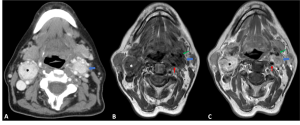
Magnetic resonance (MR) imaging is the most sensitive modality to characterize these lesions, which due to their vascular nature will typically demonstrate a “salt and pepper” appearance, relating to the presence of intratumoral hemorrhage and flow voids (Figure 2). This appearance is, however, most apparent in tumors larger than 1 cm. After administration of intravenous (IV) gadolinium contrast agent, most frequently they present avid and homogeneous enhancement (Figure 2C).
Computed tomography (CT) is useful in the case of paragangliomas involving the skull base, as it helps to evaluate the involvement of key bony structures, and to guide management. On CT, they most commonly present as a homogeneous soft tissue mass that avidly enhances after administration of IV contrast [1,3].
CT/MR angiography or digital subtraction angiography may be useful in the preoperative setting, to identify feeding vessels for planning of subsequent embolization or surgery, as well as to demonstrate the presence of multicentric disease [3].
PET/CT is recommended in patients with known metastatic disease, or when at high risk for metastasis and/or multifocal disease, as it shows superior lesion detectability when compared to CT and MR.
Accurate diagnosis of the type of head and neck paraganglioma is possible taking into consideration the anatomic location, pattern of vessel displacement, and skull base involvement.
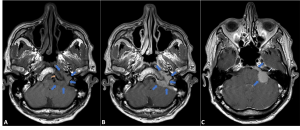
The most common location for paragangliomas in the head and neck is in the carotid body, at the carotid bifurcation, with splaying of the internal and external carotid arteries (Figure 2). The splaying of these vessels is referred to as the “lyre sign” (Figure 2D). When large enough, it can compress the adjacent nerves, resulting in dysphagia, hoarseness, or Horner’s syndrome. They are most often unilateral, but bilateral lesions can be seen in approximately 18% of patients (Figure 3). The relationship with the carotid arteries, according to the Shamblin classification, predicts resectability and risk of blood loss during surgical resection [1,3].
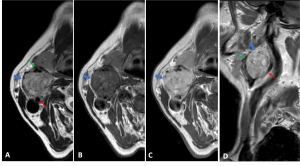
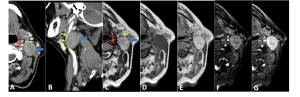
The main differential diagnosis to consider in cases where a mass is seen in this location is a peripheral nerve sheath tumor (schwannoma or neurofibroma) (Figures 4, 5). These tumors are generally less vascular and are not expected to show a “salt and pepper” appearance. The vascular behavior of the lesion can be better ascertained in a dynamic contrast-enhanced MR, where a paraganglioma will usually show a high peak enhancement with a short time-to-peak, while a schwannoma will demonstrate a low peak enhancement with a long time-to-peak. The pattern of vessel displacement also differs as, for example, a vagal schwannoma will generally splay the internal jugular vein and internal carotid artery, the latter being displaced anteromedially [3-5].
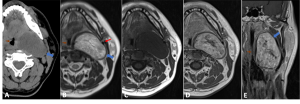
Another differential consideration is a hypervascular metastasis, where a “salt and pepper” appearance can also be seen. This should especially be considered in patients with known malignancy, such as thyroid or renal cell carcinoma (Figure 6) [3].
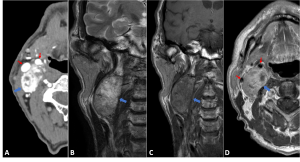
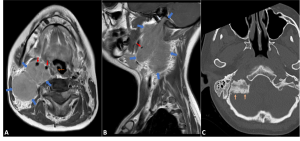
Vagal paragangliomas are less common than carotid body or jugular paragangliomas. While presenting most commonly as a slow growing painless mass, they may cause hoarseness due to vocal cord paralysis. The typical location is below the skull base and above the carotid bifurcation, although they can occur anywhere along the course of the vagus nerve. The tissue characteristics are similar to the carotid body paraganglioma, but the mass effect on the vessels differs from it, as the posterolateral position of the vagus nerve in relation to the internal and external carotid arteries results in displacement of those vessels together anteromedially, and the jugular vein posterolaterally (Figure 7). CT is of particular importance in cases of high vagal paragangliomas, to evaluate for bone involvement of the cranial base. The main differential diagnosis is a vagal schwannoma or neurofibroma [1,3].
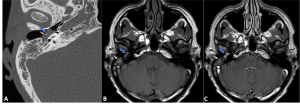
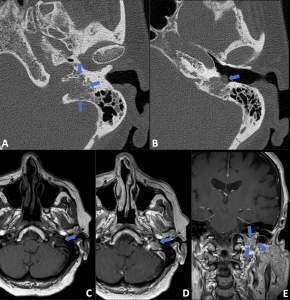
Jugular paragangliomas are the most common tumor found in the jugular foramen, and the second most common head and neck paraganglioma. Clinically, they most often present with hearing loss or unilateral tinnitus. They expand aggressively into the temporal bone, in later stages presenting with bony erosion and a “moth-eaten” appearance of the temporal bone. Extension into the middle ear may occur, as its presence indicates a jugulotympanic paraganglioma (Figure 8). In such cases, usually it is not clear whether the tumor originates from the jugular fossa or the middle ear, and they most commonly present as pulsatile tinnitus, and in some cases IX and X cranial nerves deficits. When evaluating for jugular or jugulotympanic paragangliomas, both CT and MR are indicated, as the former allows for assessment of the osseous involvement for preoperative planning, and the latter is more sensitive for intracranial extension.
The differential diagnosis of jugular paragangliomas includes other tumors originating or extending through the jugular fossa, most often schwannomas, neurofibromas, or meningiomas [1,3,6]. Peripheral neural sheath tumors are usually well-delineated enhancing lesions (Figure 9), unlike jugular paragangliomas which expand aggressively and have irregular margins. Another distinguishing feature is that neural sheath tumors usually compress the jugular vein, while jugular paragangliomas may invade it. Flow voids are not a clearly distinguishing feature, as they can be seen in certain vascular schwannomas.

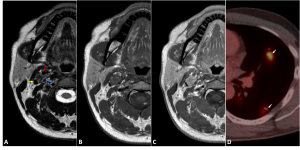
As for meningiomas, the presence of hyperostosis (which is typical for meningiomas that abut the cranial base) and the pattern of spread are some of the findings that help in the differential diagnosis (Figure 10). While jugular paragangliomas typically extend into the hypotympanum, with only limited involvement of the carotid space inferiorly, meningiomas may extend inferiorly into the nasopharynx and the carotid space (Figure 11) [3,6].
Tympanic paragangliomas are the most common tumor of the middle ear, and 80-90% of patients are women. Clinically, they most often present with pulsatile tinnitus or unilateral hearing loss, and commonly a red pulsatile mass is seen within the middle ear on otoscopic examination. On imaging, a soft tissue mass in the cochlear promontory is seen, with no dehiscence or osseous erosion around the jugular bulb. Imaging allows to differentiate from an aberrant course of the internal carotid artery, which clinically may be undistinguishable from a tympanic paraganglioma, as its injury during surgery can result in significant morbidity [1,3].
CT is the modality of choice for its evaluation, but MR may be useful to differentiate it from mimics such as inspissated secretions, cholesteatomas, or other tumors of the middle ear. Tympanic paragangliomas markedly enhance after contrast (Figure 12) due to their highly vascular nature, which helps to differentiate them from inspissated secretions or cholesteatomas, which don’t enhance.

The typical location of the tympanic paraganglioma at the cochlear promontory, as well as its pulsatile nature, which is not seen in other middle ear tumors such as a schwannoma or an adenoma, also help in the differential diagnosis (Figure 13) [3,7,8].