The novelty of the present study lies in its focus on developing a comprehensive management guideline tailored to the needs of clinicians in specific regions, such as Iraq. Despite the availability of various treatment options, gabs in the literature exist regarding the optimal managment of DDH in different regions ,Therefore, the present study aims to address the gaps by developing a regional management guideline for DDH that clinicians in Iraq and other Middle Eastern countries can use.
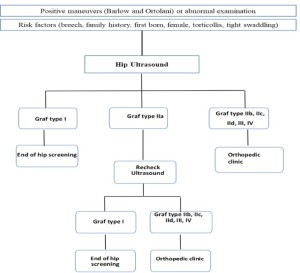
1. Pediatrician guideline : Clinical examination remains the frontline method for early detection of DDH in infants. This includes inspection, palpation and stability assessment. The use of Barlow and Ortolani maneuvers is standard practice, although their limited sensitivity [2]
2. Radiologist DDH guideline :
2.1. Ultrasound -Ultrasound is the preferred diagnostic tool for assessing the immature hip due to its ability to visualize cartilaginous components and assess hip stability dynamically. Its value decreases as the femoral head ossifies, necessitating radiography for patients older than six months [3]. Ultrasound is generally suitable for infants aged 6 weeks to 6 months.
-The indications for hip ultrasound
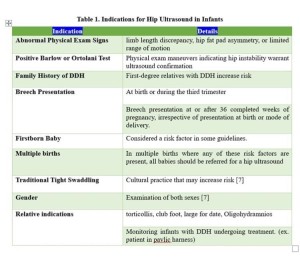
-Hip ultrasound examinations are generally not recommended for infants younger than 6 weeks of age due to the presence of physiologic laxity but may be warranted if abnormal physical examination findings are present [4].
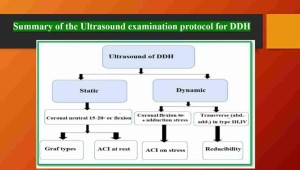
-Both hips should be examined using two orthogonal planes: coronal (standard plane) and transverse (flexed hip with and without stress).
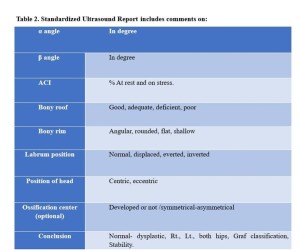
-Examination positions include supine or lateral decubitus. The coronal view assesses the femoral head position and acetabular morphology by measuring the acetabular alpha and beta angles while the transverse plane tests hip stability.



-Morphology is assessed at rest through Graf types, with acetabular coverage index (ACI) measurements. Stress maneuvers assess hip instability and are avoided in patients immobilized in a Pavlik harness or abduction splint unless specifically requested. A high-frequency linear transducer is used, with total ultrasound exposure minimized according to ALARA principles. The recommended frequency is 12-5 MHz. Techniques include static modified Graf (coronal lateral decubitus) with a neutral position of 10º-15º or flexion, and dynamic Harcke test (coronal lateral decubitus) with hip-knee flexion at 90º and adduction stress. The Morin-Terjesen technique calculates the bone coverage percentage of the femoral head(ACI). Color Doppler assesses blood flow during treatment to evaluate avascular necrosis risk [5].
-Documentation includes permanent records of the ultrasound examination with comparisons to prior imaging studies
2.2. Additional Imaging Modalities
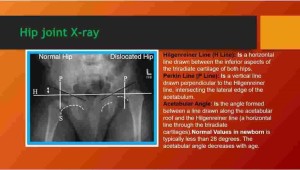
-Radiography is reserved for infants older than six months or when ultrasound evaluation is insufficient. It is used to confirm DDH suspicion, monitor the condition, or report the recovery.
-Arthrograms, CT scans, and MRIs are limited to intraoperative evaluations and post-reduction monitoring.
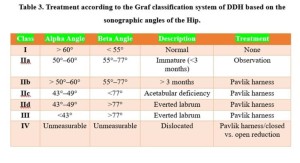
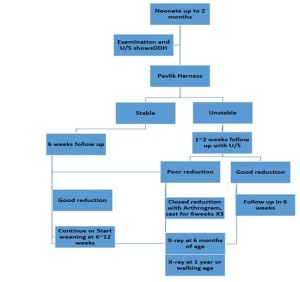
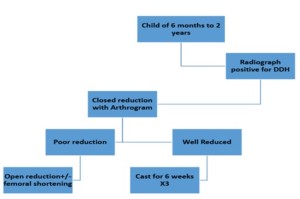
3. Orthopedic surgeon DDH guideline
- Age-specific treatment protocols aimed at establishing a stable, congruent hip joint while minimizing complications, such as avascular necrosis (AVN), nerve palsy, residual dysplasia, and gait abnormalities.
-The use of ultrasound ,particularly Graf’s Technique and Harke's dynamic assessment, is advocated for guiding management decisions. [6].