1. Imaging techniques
Imaging algorithms must cover hemorrhage exclusion, assess stroke mimics, and consider eligibility for intra-arterial therapy.
- CT: the gold standard in the acute setting enabling hemorrhagic stroke exclusion and early ischemic change detection.
- MRI: higher sensitivity with faster acquisition times. MRI protocols with DWI, gradient-echo, FLAIR sequences, MR angiography, and post-contrast perfusion, can be performed in 6-15’.
- CT/MRI angiography: provides rapid and precise vascular interpretation. Venous imaging must be included in young adults.
- Perfusion images: crucial in juvenile stroke, aiding in selecting candidates for endovascular treatment by assessing the infarct core.
- Vessel wall imaging (VWI): using black blood sequences and pre/post-contrast acquisitions, differentiates intracranial diseases by evaluating stenosis, concentric/eccentric nature, location, and enhancement.
- Conventional catheter angiography remains the gold standard for intracranial steno-occlusive diseases, non-atherosclerotic vasculopathy, and planned revascularization.
 Fig 1: Imaging techniques
Fig 1: Imaging techniques Fig 2: Imaging techniques: Vessel wall imaging
Fig 2: Imaging techniques: Vessel wall imaging Fig 3: Diagnostic approach to juvenile stroke
Fig 3: Diagnostic approach to juvenile stroke
2. Classification
According to imaging patterns, causes are classified into 5 categories.
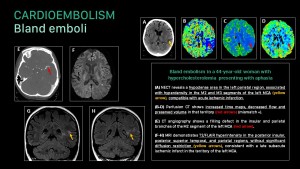
Cardioembolism
Primary cause of ischemic stroke in young individuals. Imaging reveals multifocal infarcts in various arterial territories due to emboli release or solitary embolus causing a single vascular territory infarct.
- Bland emboli
Bland emboli heighten the risk of ischemic stroke and silent cerebral infarction syndrome. Linked with cardiac masses, arrhythmias, dilated cardiomyopathy, and paradoxical thromboembolism, they typically manifest as multifocal small infarcts in various arterial territories.
Cerebral embolization caused by atrial myxoma leads to infarction, aneurysm and metastasis. Aneurysms, often multiple and hyperdense on non-contrast CT (mixoid matrix, wall calcification), favor MCA distal branches. Metastases appear as multiple, typically frontoparietal hemorrhagic masses.
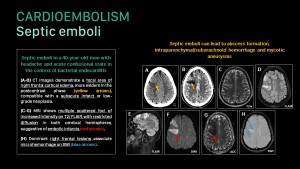
- Septic Emboli
Septic emboli, linked to endocarditis, most commonly course with small scattered ischemic infarcts. Other findings: abscesses, intraparenchymal/subarachnoid hemorrhage, and mycotic aneurysms.
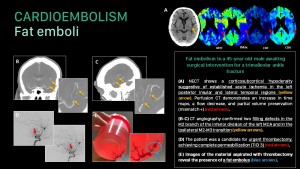
- Fat Emboli
Cerebral fat embolism syndrome tends to develop in patients with large displaced fractures or sickle cell anemia.
Acute phase: MRI shows a "starfield" pattern with multiple scattered foci of diffusion restriction and FLAIR hyperintensity in the white matter, corpus callosum, basal ganglia, thalamus, brainstem, and cerebellum.
Subacute phase: confluent areas of diffusion restriction appear in subcortical and deep white matter. Microhemorrhages in areas of cytotoxic edema or more extensive may appear.
- Air emboli
Air emboli result from invasive procedures causing contact between the external environment and the vascular system under an atmospheric pressure gradient. Proximal introduction before aortic branching leads to scattered infarcts across multiple vascular territories. Air introduction in carotid/vertebrobasilar procedures restricts infarcts to a specific vascular territory.
Large vessel vasculopathy
- Atherosclerosis
Atherosclerosis, uncommon in young individuals, is linked to cardiovascular risk factors, causing thromboembolic, hypoperfusion, or mixed strokes.
CT/MR angiography reveals calcified/non-calcified atherosclerotic plaques with stenosis, while VWI highlights eccentric wall enhancement. Plaque features like ulceration, fibrous cap thickness, and necrotic core predict stroke.
- Dissection
Cervical arterial dissection, a major cause of juvenile stroke, may be spontaneous or traumatic, involving thromboembolic stroke (80%), hypoperfusion, and mixed mechanisms. Up to 10% experience bilateral dissection.
CT/MR angiography reveals irregular filiform stenosis (string of pearls sign), narrowing to a point (flame sign), mural thickening (crescent sign), or an intimal flap.
T1-weighted FS MR is the most sensitive sequence, with the hematoma hypointense in T1 and T2 in the hyperacute phase and hyperintense in T1 in the subacute phase, with the residual lumen as a flow void. Pseudoaneurysms can form in the subacute phase.
Intracranial dissection, rarer but with increased aneurysm and extravascular hemorrhage risk, features a curvilinear hyperintensity (intimal flap), eccentric thickening with blood signal (intramural hematoma), and post-contrast T1 enhancement in vessel layers.
- Radiation-induced arteriopathy
Radiation induces morphological features akin to atherosclerosis. Vascular injury can result in severe carotid artery stenosis and stroke/TIA related to thromboembolism or hypoperfusion.
Head radiation causes large vessel stenosis, moyamoya pattern, cavernous malformations, aneurysms, and capillary telangiectasias.
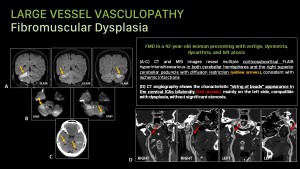
- Fibromuscular Dysplasia (FMD)
After renal arteries, extracranial internal carotid and vertebral arteries are the most frequent locations. FMD exhibits alternating stenosis and dilatations, creating a “string of beads” appearance. Less frequent findings: vascular loops, fusiform vascular ectasia, dissection, and aneurysms that can lead to TIA, stroke, and subarachnoid hemorrhage.
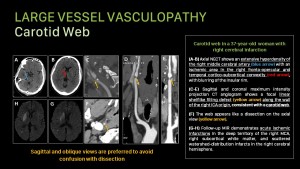
- Carotid Web
Fibrous thickening in the carotid intima causes blood stasis and thrombus formation, leading to ischemic stroke, especially in the anterior circulation.
CT/MR angiography displays a thin, linear non-enhancing membrane extending from the posterior aspect of the carotid bulb into the lumen, without wall thickening.
Small vessel vasculopathy
Lacunar infarcts are uncommon in young people and are associated with cardiovascular risk factors.
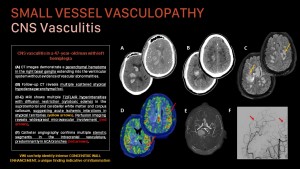
- CNS Vasculitis
Primary CNS vasculitis is an idiopathic inflammatory disease of small/medium-sized arteries affecting the nervous system. Secondary CNS vasculitis comprises systemic vasculitis secondary to different conditions.
VWI can help identify intense concentric wall enhancement, a unique finding indicating inflammation. Other features include multifocal infarcts, parenchymal/subarachnoid hemorrhage, leptomeningeal enhancement, white matter edema, and beaded arterial appearance.
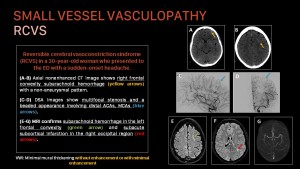
- Reversible Cerebral Vasoconstriction Syndrome (RCVS)
RCVS presents with recurrent thunderclap headaches and reversible segmental and multifocal cerebral artery vasoconstriction, resolving within 8-12 weeks.
Initial diagnosis involves CT/MR angiography. Conventional angiography as the gold standard for distal vessel vasoconstriction.
Characteristic findings include bilateral tapering of medium-sized arteries, followed by abnormally dilated second and third-order branches. VW-MR images may show absent/mild vascular wall enhancement. Additional features: wathershed infarcts, convexity subarachnoid hemorrhage, and intraparenchymal hemorrhage.
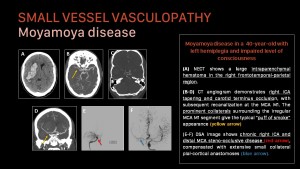
- Moyamoya Disease
A progressive idiopathic steno-occlusive, non-inflammatory, and non-atherosclerotic disorder affecting the terminal ICA and proximal ACA/MCA segments with relative PCA preservation.
Catheter angiography is the gold standard for intracranial evaluation.
Steno-occlusive changes prompt compensatory collateral development, creating the characteristic "puff of smoke" appearance on angiography. It leads to ischemic infarctions from arterial occlusion and hemorrhages from arterial rupture.
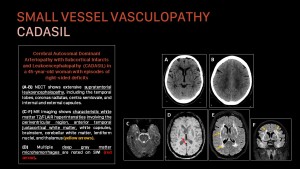
- Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL)
Most common monogenic disorder (caused by NOTCH3 gene mutations) causing stroke and vascular dementia.
MRI: symmetrical T2/FLAIR white matter hyperintensities (periventricular, anterior temporal poles, external capsules, sparing subcortical U fibers), subcortical infarcts, and deep cerebral microhemorrhages, sparing the fronto-orbital and occipital regions.
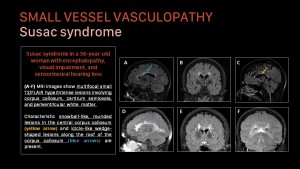
- Susac Syndrome
Susac Syndrome features small multifocal T2/FLAIR white matter hyperintensities, including snowball-like lesions in the central corpus callosum and icicle-like wedge-shaped lesions along its roof. Deep gray matter, cerebellum, and brainstem may be affected.
Lesions result from arteriolar infarction, showing restricted diffusion in acute and subacute phases, subacute enhancement, and chronic cavitation. Leptomeningeal enhancement occurs in 30%.
- Infection
The underlying mechanisms include vasculitis, meningitis, cardioembolism, arachnoiditis, arterial compression, and occlusion. Imaging findings depend on the mechanism and affected areas.
Toxic-metabolic
- Mitochondrial Encephalopathy with Lactic Acidosis and Stroke-like Episodes (MELAS)
A mitochondrial disorder characterized by pseudo-seizures, seizures, and lactic acidosis.
CT/MRI: shows strokelike lesions in different stages of evolution, predominantly in the parietal, temporal, and occipital lobes, along with basal ganglia calcifications and brain atrophy.
Spectroscopy indicates elevated lactate peaks.
- Drug Abuse
Major cause of ischemic stroke in young adults, concerning hypertension, arrhythmias, vasospasm, vasculitis, thrombosis, cardioembolism, and injected material embolization, leading to encephalopathy, hemorrhage, or ischemic infarction.
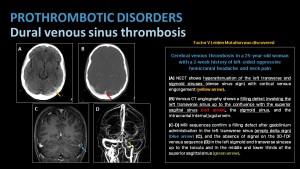
Hypercoagulable Disorders
Hypercoagulability can lead to arterial infarctions via thromboembolism, intracardiac shunts, or venous infarctions.
Prothrombotic disorders include Antiphospholipid syndrome, Factor V Leiden Mutation, oral contraceptive use, Pregnancy, and peripartum.
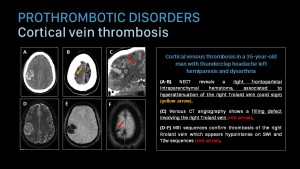
- Venous thrombosis
CT is the initial evaluation choice, while MRI is preferred for follow-up.
Dural venous thrombosis is evident as hyperdensity of major dural sinuses and/or cortical veins on non-contrast CT (dense sinus sign, cord sign), absence of hypointense flow voids on T2-weighted susceptibility-weighted MRI, or lack of enhancement in dural sinuses or cortical veins on CT/MR venography and certain contrast-enhanced T1-weighted 3D MRI sequences.
Indirect signs of venous drainage obstruction include vasogenic edema, cytotoxic edema, and intraparenchymal hemorrhage. Other findings include falx/tentorium enhancement, subdural hematoma, and subarachnoid hemorrhage.