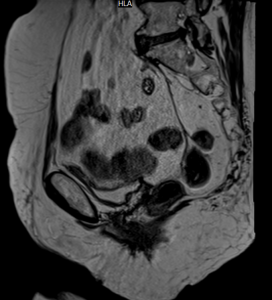
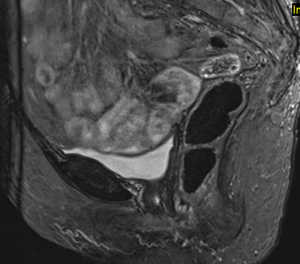
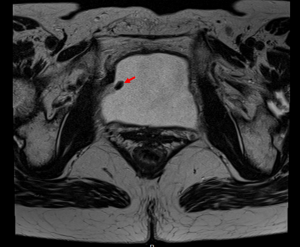
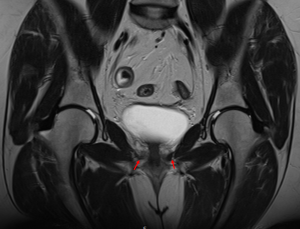
Rectopexy
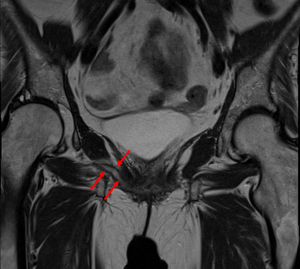
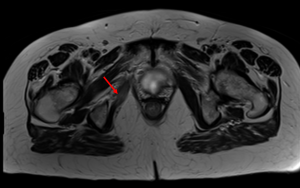
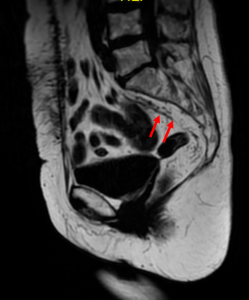
The mesh is secured to the rectal wall and suspended superiorly from the sacral promontory. In women, the mesh can also attached to the superior vagina for additional support [5]. (Figures 1-3)

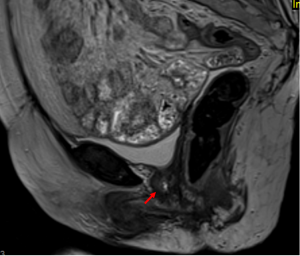
Rectopexy Complications
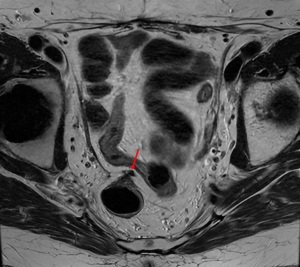
The rectopexy mesh can cause secondary adhesions to the surrounding tissues and in more severe cases, fistulation. This example shows fibrotic changes at the insertion points as well as tethering of the rectum and vaginal vault. (Figure 4)
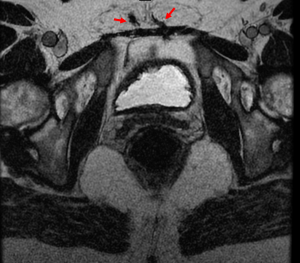
Tension-free Vaginal Tape (TVT)
TVT involves creating a sling underneath the urethra to provide support for stress incontinence. The sling comprises of two ‘arms’ which should traverse through the rectus muscles, above the pubis. Each arm runs in the retropubic space with a clear fat plane between the urinary bladder. [6] Posteriorly, the tape courses into the urethrovaginal space (where it may always not be seen). (Figure 5 -7).


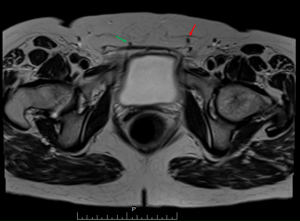
TVT Complications
Complications that may arise include misplacement, infection, mesh extrusion into the bladder, urethra or vagina.
The first TVT case shows the left subcutaneous arm is misplaced – compared to the right arm (green arrow) it lies more laterally and this can cause compromise of the ilioinguinal nerve. The patient had symptoms of constant groin pain. (Figure 8)
The next patient was experiencing dysuria – the MRI shows urethral extrusion with focal oedema surrounding the urethra. Extrusion was confirmed on cystoscopy. (Figure 9 and 10).
Another example of extrusion, this time involving the bladder – the right arm of the tape is thickened and inflamed with clear extrusion into the bladder, also confirmed on cystoscopy. (Figure 11 and 12).

Transobturator Tape (TOT)
The TOT was developed after the TVT to reduce the risk of bladder injury [7]. The tape has a transverse course and can often be difficult to visualise on MRI in the absence of any complications. It should pass above and through the obturator foramen, under the levator ani and pelvic fascia and then continue in the urethrovaginal space [8]. (Figure 13).
TOT Complications
The potential TOT complications are similar to those already discussed – this example shows marked inflammation of the right arm of the TOT with secondary oedema and inflammation of the right obturator internus muscle (Figure 14-16).