Definition : Rasmussen encephalitis, or chronic focal encephalitis, is a chronic inflammatory disorder of unknown origin that mainly affects one hemisphere of the brain. While 85% of cases occur in children under 10, more adult cases are being identified through routine MRI for intractable seizures [1].
Mechanism : The exact cause remains unclear; however, various viral infections and inflammatory events have been proposed as triggers, alongside a suggested autoimmune mechanism.
Clinical features :
Rasmussen encephalitis progresses through three clinical phases [2].
-
Prodromal phase
- Occasional focal seizures.
- Mild neurological symptoms, such as slight hemiparesis.
-
Acute phase
- Frequent drug-resistant seizures, including epilepsia partialis continua and focal-to-bilateral tonic-clonic seizures.
- Worsening neurological deficits, such as hemiparesis, dysphasia (if the dominant hemisphere is involved), or homonymous hemianopia.
- Possible cognitive decline.
-
Chronic (residual) phase
- Persistent focal epilepsy that does not respond to treatment.
- Permanent neurological deficits and cognitive impairment.
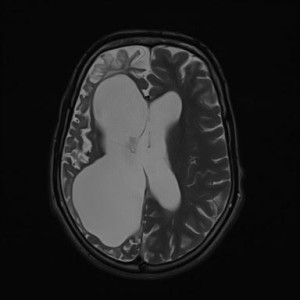
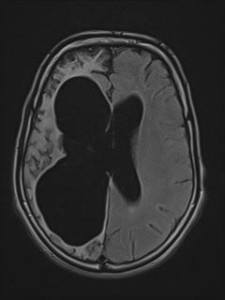
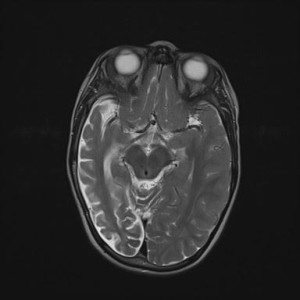
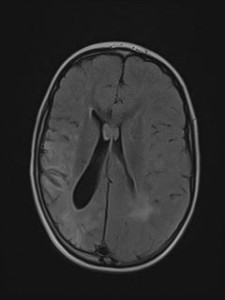
MRI findings : Initial atrophy is seen in the ipsilateral caudate nucleus, progressing to more widespread atrophy and signal changes in the affected hemisphere.
The imaging characteristics include [3]:
- T1 : Unilateral cortical atrophy with ex vacuo ventricular dilatation.
- T2 / FLAIR : Hyperintense signal in cortical and subcortical regions.
- DWI/ADC: Restricted diffusion in altered signal areas.
- T1 with contrast : No significant post-contrast enhancement.
Differential diagnoses :
- Dyke-Davidoff-Masson syndrome :
Condition characterized by hemicerebral atrophy/hypoplasia secondary to brain insult usually in fetal or early childhood period and is accompanied by ipsilateral compensatory osseous hypertrophy and contralateral hemiparesis.
It is characterized by:
-
Thickening of the skull vault (compensatory)
-
Enlargement of the frontal sinus (also ethmoidal and mastoid air-cells)
-
Elevation of the petrous ridge
-
Ipsilateral falcine displacement
-
Capillary malformations (are a novel finding for children with Dyke-Davidoff-Masson syndrome)
-
- Sturge-Weber syndrome :Also referred to as encephalotrigeminal or encephalofacial angiomatosis, this phakomatosis is marked by a facial port-wine nevus (capillary malformation) and pial angiomas. It falls within the broader spectrum of cerebrofacial arteriovenous metameric syndrome (CAMS) phenotypes.
It is characterized by:
- Subcortical calcification, associated withparenchymal volume loss
- Tram-track sign of cortical and subcortical calcification.
- Possible calvarial and regional sinus enlargement.
- Enlargement of ipsilateral choroid plexus.
- Asymmetric cavernous sinus enlargement
- Unilateral megalencephaly.