Complaint of focal lesions on the fingers, often palpable and visible, is common among patients. Ultrasound has become established as a fundamental method in the evaluation of hand and finger pathologies, providing accessible and non-invasive diagnostic guidance for a variety of conditions, including traumatic, inflammatory, and neoplastic lesions.
High-frequency transducers allow detailed visualization of superficial anatomical structures, aiding in differential diagnosis and clinical management. Therefore, radiologists must be familiar with the main imaging patterns of focal lesions of the fingers , as well as with relevant differential diagnoses.
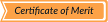
Synovial Cysts
Synovial cysts are the most common cystic lesions of the hand and fingers. They result from herniation of synovial fluid and synovial lining through a defect in the joint capsule or tendon sheath, creating a communication with the adjacent joint. Clinically, patients often present with a slow-growing, painless, palpable mass, although nail deformity or discomfort may occur when located near the distal interphalangeal joint.
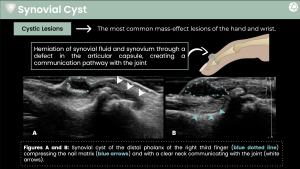
On ultrasound, synovial cysts appear as well-defined, anechoic or hypoechoic cystic lesions, often multilocular, with posterior acoustic enhancement. A key diagnostic feature is the presence of a narrow neck or tract communicating with the joint, best visualized with dynamic scanning. Doppler examination typically shows no internal vascularity, although mild peripheral flow may be present due to reactive changes.
Mucoid Cysts
Mucoid cysts represent mucoid degeneration of periarticular connective tissue, with accumulation of collagen degradation products. Unlike synovial cysts, they do not communicate with the joint. They most commonly affect the distal interphalangeal joint region and periungual tissues and are frequently associated with nail plate deformity.
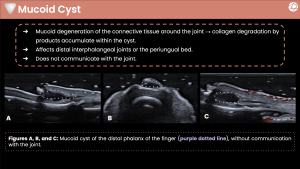
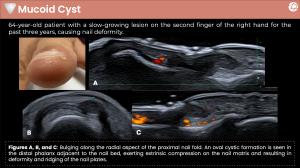
Clinically, mucoid cysts present as slow-growing, firm nodules, often causing longitudinal ridging or dystrophy of the nail. On ultrasound, they appear as well-circumscribed cystic lesions adjacent to the nail bed or matrix, typically anechoic or mildly hypoechoic, without a visible joint connection. Posterior acoustic enhancement is common, and Doppler imaging shows no internal vascularity.
Hemangiomas
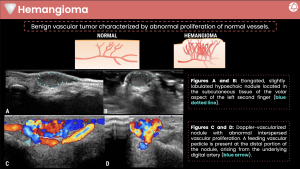
Hemangiomas are benign vascular tumors characterized by abnormal proliferation of blood vessels. They may present at any age and commonly manifest as soft, compressible masses that may increase in size with dependency or Valsalva maneuver. Pain or functional limitation may occur depending on size and location.
Ultrasound typically demonstrates a hypoechoic or heterogeneous, lobulated soft-tissue mass located in the subcutaneous tissues. Color and power Doppler reveal prominent internal vascularity, often with low-resistance arterial flow and, in some cases, identifiable feeding vessels arising from digital arteries. Phleboliths, when present, appear as echogenic foci with posterior shadowing.
Pyogenic Granulomas
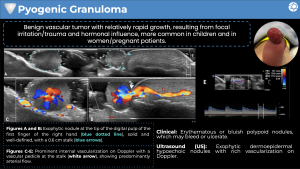
Pyogenic granulomas are benign vascular proliferations resulting from exaggerated reparative responses to trauma, irritation, or hormonal influences. They are more common in children and pregnant women and present clinically as rapidly growing, erythematous or bluish exophytic nodules that bleed easily.
On ultrasound, pyogenic granulomas appear as well-defined, hypoechoic dermoepidermal or subcutaneous nodules, frequently pedunculated. Doppler imaging demonstrates marked hypervascularity, often with a dominant vascular pedicle at the stalk and predominantly arterial flow. These features help distinguish pyogenic granulomas from other superficial soft-tissue lesions.
Glomus Tumors
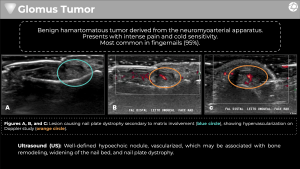
Glomus tumors are benign hamartomatous lesions arising from the neuromyoarterial receptors of the glomus body, which regulates thermoregulation. They classically present with a triad of severe localized pain, cold sensitivity, and point tenderness, most commonly involving the subungual region.
Ultrasound findings include a small, well-defined, hypoechoic nodule beneath the nail bed, often associated with nail matrix involvement and nail plate dystrophy. Color Doppler shows intense internal vascularity, a hallmark feature. Subtle cortical remodeling of the distal phalanx may also be detected, reinforcing the diagnosis.
Peripheral nerve sheath tumors are predominantly benign lesions, mainly schwannomas and neurofibromas, arising from peripheral nerves. High-frequency ultrasound (HFUS) is particularly useful for characterizing nerve continuity, encapsulation, fascicular involvement, and vascularity, aiding accurate differentiation and clinical management.
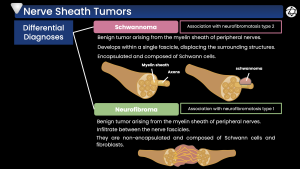
Schwannomas
Schwannomas are benign peripheral nerve sheath tumors composed exclusively of Schwann cells. They arise eccentrically from a single nerve fascicle and displace adjacent nerve fibers. Clinically, they present as slow-growing, painless masses, although paresthesia or Tinel’s sign may be elicited.
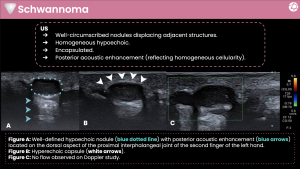
On ultrasound, schwannomas appear as well-circumscribed, encapsulated, homogeneous hypoechoic nodules, typically oval or round. They often demonstrate posterior acoustic enhancement, reflecting their uniform cellularity. The parent nerve may be visualized entering and exiting the lesion eccentrically. Doppler vascularity is variable and often minimal.
Neurofibromas
Neurofibromas are benign tumors composed of Schwann cells, fibroblasts, and perineural cells. Unlike schwannomas, they are non-encapsulated and infiltrate between nerve fascicles. They may occur sporadically or in association with neurofibromatosis type 1.
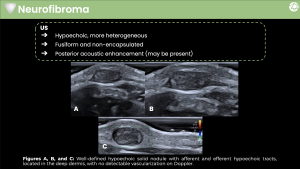
Clinically, neurofibromas present as soft, slow-growing masses and may be associated with neurologic symptoms. On ultrasound, they appear as fusiform, hypoechoic solid lesions with more heterogeneous echotexture than schwannomas. A characteristic finding is the presence of afferent and efferent nerve segments, giving a “continuity with the nerve” appearance. Posterior acoustic enhancement may be present, while Doppler flow is usually absent or minimal.
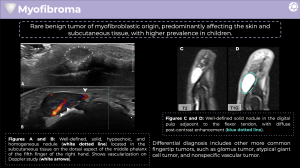
Myofibroma
Myofibroma is a rare benign tumor of myofibroblastic origin, predominantly affecting infants and children but occasionally seen in adults. It may involve the skin, subcutaneous tissues, or deeper structures and can clinically mimic other fingertip tumors.
Ultrasound typically shows a well-defined, solid hypoechoic mass, usually homogeneous, located in the subcutaneous tissue or digital pulp. Unlike many other benign finger lesions, myofibromas often demonstrate internal vascularity on Doppler imaging, which may lead to diagnostic confusion with vascular tumors. Correlation with clinical age and lesion location is therefore essential.
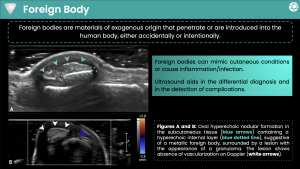
Foreign Body
Foreign body granulomas result from a chronic inflammatory reaction to retained exogenous material, such as wood, metal, or glass. Patients may not recall the inciting trauma, and the lesion may mimic infection or neoplasm.
On ultrasound, foreign bodies appear as hyperechoic linear or nodular structures with posterior acoustic shadowing, comet-tail artifacts, or reverberation, depending on their composition. Surrounding hypoechoic inflammatory tissue representing granuloma formation is commonly seen. Doppler imaging usually shows absent internal vascularity, although peripheral hyperemia may be present in active inflammation.
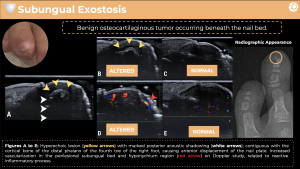
Subungual Exostosis
Subungual exostosis is a benign osteocartilaginous proliferation arising from the dorsal aspect of the distal phalanx, most commonly affecting adolescents and young adults. Clinically, it presents as a painful subungual mass causing nail plate elevation and deformity.
Ultrasound demonstrates a hyperechoic bony protuberance continuous with the cortical surface of the distal phalanx, producing marked posterior acoustic shadowing. Reactive hypervascularity of the adjacent nail bed and hyponychium may be observed on Doppler imaging, reflecting secondary inflammation. Correlation with radiographs confirms the osseous origin.