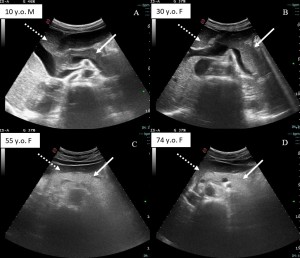
To visualize the pancreatic region in adults a convex-type US transducer with low frequencies (3.5-5 MHz) should be used. To analyze every part of the pancreatic gland transverse and oblique scans of the epigastric region should be performed. The transplenic approach can be used to explore the tail [5,6]. The pancreas has a "horse-shoe" shape, it is located at the front of the spine, it has a homogeneous structure and it is bordered by peripancreatic adipose tissue that appears hyperechoic compared with the glandular parenchyma [6]. The echostructure of the pancreas, however, changes with age. In young patients, it may be more hypoechoic than the liver parenchyma, while with aging and in obese patients, due to adipose infiltration, a greater glandular echogenicity is generally observed (Figure 1)[5]. Generally, the anteroposterior diameter of the pancreas should not exceed 20-22mm but its size can vary under normal conditions, according to age, sex and physical constitution. In particular, its overall size decreases with age in relation to the physiological tendency of parenchymal atrophy (Figure 1)[5].
The US findings of AP can be classified into 3 groups:
- Pancreatic signs
- Peri-pancreatic signs
- Associated signs
- Pancreatic signs
Pancreatic signs are not always visible, for example, in 30% of oedematous pancreatitis the US examination results negative [7]. Features that should be checked in the US evaluation of pancreatic gland in AP are:
- Pancreatic gland size: an anteroposterior diameter greater than 23 mm should be considered pathological, with measurement made in the glandular body, in a transverse plane at the level of the superior mesenteric artery (Figure 2A and 2C) [7]. However, sometimes, the enlargement can affect only the pancreatic head [8].
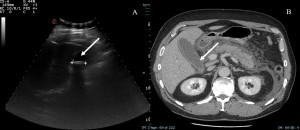
 Fig 2: US and CT image of a 76 years old male with acute pancreatitis. The pancreatic gland is increased in size (A and C, white arrows). Under the pancreas there is the formation of a fluid collection (B and D, white arrows).
Fig 2: US and CT image of a 76 years old male with acute pancreatitis. The pancreatic gland is increased in size (A and C, white arrows). Under the pancreas there is the formation of a fluid collection (B and D, white arrows). - Parenchymal echogenicity: edema that accumulates in the glandular interstitium results in a decreased parenchymal echogenicity (Figure 3) [8]. It can be compared with liver echogenicity, but this evaluation may be more difficult in patients with hepatic steatosis, misleading the diagnosis. The extent of hypoechogenicity is less pronounced in the presence of chronic pancreatitis, elderly patients, or pancreatic lipomatosis [7].
- Glandular heterogeneity and focal alterations: a heterogeneous structure is considered pathological, but the alteration can also affect a focal area creating the so-called “mass-like” lesions that are usually hypoechogenic. Such inflammatory masses pose problems of differential diagnosis with solid tumors but this finding must be associated with clinical or peri-pancreatic signs [7]. Also, necrotic foci, fluid collection and hemorrhages could be seen as focal changes [8].
- Alteration of the pancreatic duct: the Wirsung’s duct may not be recognizable because of the compressive effect of the edema or it may be dilated in patients with chronic pancreatitis or with an obstruction of the duct (e.g., from lithiasis or focal inflammation) (Figure 3) [5].
 Fig 3: US image and CT image of a 67 years old male with acute pancreatitis. The Wirsung’s duct appears dilated (A and B, white arrow), the echogenicity of the gland is decreased due to edema, and peri-pancreatic fluid collections are present (A and B, white dotted arrow).
Fig 3: US image and CT image of a 67 years old male with acute pancreatitis. The Wirsung’s duct appears dilated (A and B, white arrow), the echogenicity of the gland is decreased due to edema, and peri-pancreatic fluid collections are present (A and B, white dotted arrow).
- Peri-pancreatic signs
The most common peripancreatic findings in patients with AP are retroperitoneal inflammation (about 60%) and fluid collections (about 25%) [7]. The inflammation can be visualized as hypo- or anechogenic thickening of adipose tissue, with linear morphology. Signs of extra-pancreatic inflammation should be searched ventral to the gland, along the transverse mesocolon, and in the omental fat. Perivasal inflammation is also possible and the vessels most commonly involved are the superior mesenteric vein and splenic vein [7]. Fluid collections can be either full of hypoechoic liquid, or more complex and heterogeneous, with necrotic and hemorrhagic components (Figure 2B, 2D and 3). They can be found in the peri-glandular area but also in the small omentum, in both perirenal space (the left space more frequently affected than the right), in the anterior and posterior pararenal space and in Gerota's fascia [8]. Special attention should be paid to the detection of free endoperitoneal effusion and pleural effusion [5]. One of the most important structures to explore is the bile ducts to recognize the presence of lithiasis. Patients with choledochal lithiasis aggregate may benefit from Endoscopic Retrograde Cholangiopancreatography (ERCP), which should be performed within 48 hours of symptom onset (Figure 4) [5].
- Associated signs
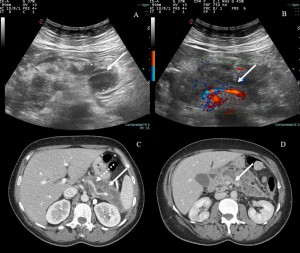
One of the most potentially fatal complications of AP is the formation of pseudoaneurysms due to the proteolytic action of pancreatic enzymes to the vascular walls because their rupture can lead to retroperitoneal hemorrhage (Figure 5C). The most affected artery is the gastroduodenal, followed by the pancreaticoduodenal and splenic. In B-mode US examination, pseudoaneurysms may appear as hypo-anechoic, rounded formations with well-defined margins simulating a small cystic lesion. Color-Doppler evaluation can show a typical "yin-yang'' circular flow pattern. When thrombosis of the pseudoaneurysm occurs, there may be a partial or complete lack of flow at Color-Doppler [6,7]. The most common vascular complication associated with AP is venous thrombosis, which may be due to peripancreatic inflammation or mass effect (Figure 5).