Accordion Sign
The Accordion Sign is a radiological feature indicative of pseudomembranous colitis, characterized by alternating thickened colonic mucosa and intraluminal contrast, mimicking the appearance of an accordion. It reflects severe colonic inflammation and edema. On CECT imaging, this sign manifests as exaggerated haustral folds with hyperattenuating contrast or stool between them, often accompanied by colonic wall thickening and fat stranding. [2]
Associated with Clostridioides difficile infection, this sign facilitates early diagnosis and timely intervention, including targeted antibiotic therapy, reducing risks of complications.
Kawamoto et al. first detailed this sign in 1999, correlating it with clinical and pathological findings.
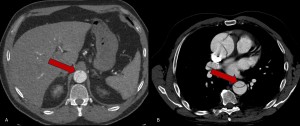
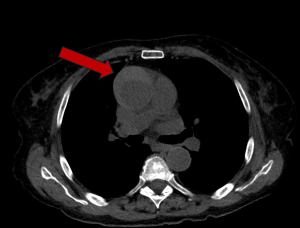
Bird Beak Sign
This sign, observed in hollow organs or parenchymal structures, reflects abrupt luminal narrowing resembling a bird’s beak. In this context, a mass deforms the contour of an adjacent organ, producing a "beak-like" appearance, suggesting that the mass originates from the organ itself. [3]
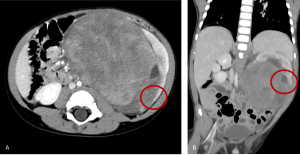
It also appears in aortic dissection as the acute angle between the dissection flap and the the adventitia of the remaining wall. This sign can be clearly visualised on CECT.
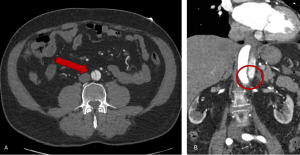
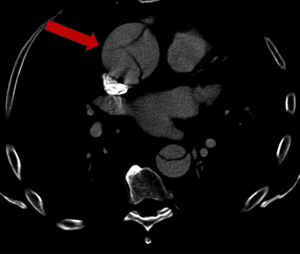
Blush Sign
This sign indicates active hemorrhage, characterized by contrast extravasation outside vascular confines.
On CECT, it appears as curved areas of contrast enhancement >1 mm × 2 mm, which grow in size and density during delayed imaging phases.
This sign was initially documented by S.C. Schein in 1979. [4]
Cobweb Sign
Indicative of chronic aortic dissections, this sign consists of thin, linear remnants of the medial layer in the false lumen. These filaments reliably differentiate the false lumen from the true lumen on CT.
This sign was first described by Williams et al. [5,6]
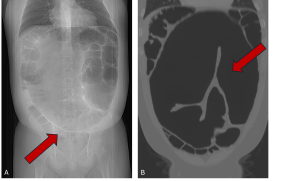
Coffee Bean Sign
A hallmark of sigmoid volvulus, the coffee bean sign features a closed-loop sigmoid colon with a characteristic convexity typically oriented toward the right upper quadrant. It reflects bowel obstruction. The earliest description of this sign is credited to Rigler in 1941. [7]
CT imaging provides additional accuracy, delineating the closed-loop structure and pinpointing the transition point at the site of torsion. Early identification prevents serious complications like ischemia, necrosis, or perforation. [8]
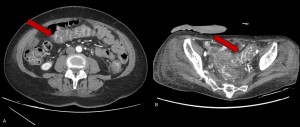
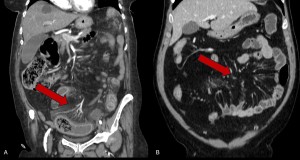
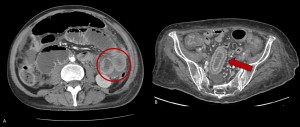
Comb sign
The Comb Sign is a radiological marker frequently linked to Crohn's disease but also observed in other acute inflammatory bowel conditions and mesenteric vasculitis. Most evident on CECT, the sign represents mesenteric vascular congestion due to fibrofatty proliferation and inflammatory infiltrates. [9]
It features dilated and engorged mesenteric vessels arranged linearly and radiating from the bowel, resembling the teeth of a comb, accompanied by mesenteric fat stranding and bowel wall edema. Initially described by Madureira in 2004, this sign underscores mesenteric inflammation typical of active Crohn’s disease. [10]
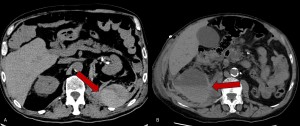
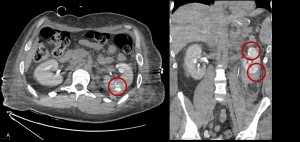
Cortical rim sign
It is a radiological marker indicative of renal infarction. It was first described in 1974 and resembles the visual effect of a solar eclipse. [11]
This sign presents as a thin (~3 mm) enhancing rim of viable subcapsular cortex. The enhancement is attributed to collateral vessels perfusing the outer rim of the renal cortex in cases of main renal artery occlusion.
Typical features include: Wedge-shaped, low-attenuation areas with the apex directed toward the renal sinus. The Cortical rim sign observed in approximately 50% of renal infarcts. [12]

Hematocrit Sign
Observed on non-contrast CT, the hematocrit sign indicates hemorrhage or focal bleeding. It is depicted as a separation of blood components, where denser corpuscular elements (>60HU) settle, forming a fluid-fluid level.
The sign was first described by Swenson et al. in 1984. [13]
Hyperdense Crescent Sign
Seen in abdominal aortic aneurysms (AAA), this sign denotes blood dissecting into an unstable mural thrombus or aneurysmal wall.
On non- contrast CT it appears as a crescent-shaped hyperattenuated area located along the aortic wall or within the mural thrombus. This radiological sign is highly specific for an impending rupture.
The Hyperdense Crescent Sign was first recognized in the early 1990. [14]
Mercedes-Benz Sign
A rare manifestation of chronic aortic dissection, the sign depicts three lumens separated by intimal flaps, resembling the triradiate Mercedes-Benz logo. [15]
First described in the 1980. It signifies advanced dissection stages with a risk of complications like thromboembolism and rupture. [16]
Paper-Thin Wall Sign
Associated with advanced ischemic injury, this sign is marked by a thin, hypodense bowel wall with reduced or absent enhancement, often accompanied by pneumatosis intestinalis. The sign highlights irreversible ischemic damage caused by transmural infarction. [17]
Sandwich Sign
This sign, first described by Swischuk in 1985, is most commonly associated with intussusception, observed on longitudinal CT scans. It describes the appearance of one intestinal segment (intussusceptum) telescoping into another (intussuscipiens), creating a layered configuration like a sandwich. [18,19]
However similar imaging features can be seen in intestinal lymphoma, where enlarged lymph nodes and thickened intestinal walls mimic the layered structure.
CT Features
- Outer layers ("bread") formed by the walls of the intussusceptum and intussuscipiens.
- Inner filling: Composed of mesenteric fat and vessels extending into the intussusceptum.
On CECT, mesenteric vessels appear elongated or displaced within the intussusceptum, while intravenous contrast accentuates the intestinal walls. This technique is particularly valuable for detecting vascular compromise. [20]
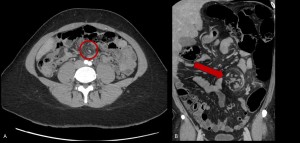
Striated nephrogram - Ragged fan Sign
Described by Bigongiari et al. in 1975, the striated nephrogram is most commonly associated with acute pyelonephritis. [21] It may also occur in conditions like renal vein thrombosis, renal contusion, or ureteral obstruction.
Appearance: Alternating low- and normal-density bands with a radial, wedge-shaped distribution on parenchymal-phase contrast enhancement. Low-density bands represent either contrast-agent-free collecting ducts or interstitial edema between contrast-filled nephrons. [22]
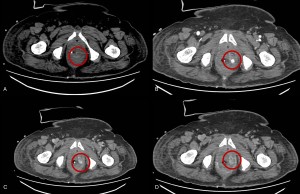
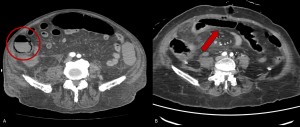
Target Sign
Also termed the doughnut sign, this finding features concentric layers of variable attenuation within the bowel wall. It appears in conditions such as ischemia, appendicitis, intussusception and Crohn’s disease. [23]
- Bowel Ischemia
In the early stages, particularly venous or transient ischemia, the target sign reflects bowel wall edema. CECT, the diagnostic gold standard, reveals a stratified appearance due to edema and hyperemia. This sign indicates the reversible nature of ischemic bowel injury. [24]
- Inner hyperdense layer: Hyperemic or ischemic mucosa.
- Intermediate hypodense layer: Submucosal edema.
- Outer hyperdense layer: Muscularis propria.
Cross-sectional imaging of affected bowel segments shows these layers, with advanced disease potentially exhibiting transmural hyperattenuation due to hemorrhage. [25]
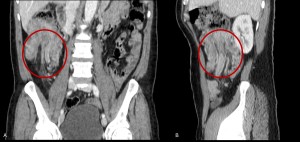
- Intussusception
The target sign, a defining feature of intussusception, presents as a concentric layers formed when one segment of the intestine telescopes into an adjacent segment. This condition is most commonly seen in pediatric patients. [26]
In adults or complicated cases, CT is often employed. On CT, the target sign appears on axial views as intestinal wall thickening with alternating hyperdense (mucosa and muscularis propria) and hypodense (submucosa) rings. [27]

Whirlpool Sign
This sign, indicative of volvulus, shows twisted mesenteric vessels spiraling around a fixed axis. It is crucial for diagnosing bowel ischemia and torsion pathologies. [28]
This radiological finding, resembling a whirlpool, is best observed on axial CECT images. Key imaging features include:
- Twisting of the superior mesenteric vein (SMV) around the superior mesenteric artery (SMA).
- Dilated proximal bowel loops and collapsed distal segments.
- Signs of ischemia or necrosis, such as bowel wall thickening, fat stranding, and pneumatosis intestinalis. [29]
First described by Fisher in 1981 in pediatric patients with small bowel volvulus, the Whirlpool Sign’s applications expanded with the adoption of CT imaging in the 1990s, including its relevance to sigmoid volvulus. Nakamata provided a multi-planar imaging for increased diagnostic sensitivity in torsion-related pathologies. [30,31]
Windsock Sign
Common in aortic dissection, this sign is formed by a circumferentially detached intimal flap that freely oscillates in the aortic lumen, indicative of severe dissection. [32]
This sign was first described by Fisher et al. (1994). [33]

Yin-Yang Sign- Pepsi Sign
The Yin-Yang Sign, also called Pepsi Sign, is a distinctive radiological feature of aneurysms, characterized by contrasting densities within the aneurysmal sac. These densities represent flowing blood (high density) and stagnant blood or mural thrombus (low density), forming a pattern reminiscent of the yin-yang symbol. [34] This sign is commonly observed in pseudoaneurysms and partially thrombosed aneurysms, making it particularly useful in assessing flow dynamics.
CECT highlights the contrast between the patent lumen and mural thrombus. [35]
