Findings and procedure details
To illustrate the spectrum of abdominal and pelvic manifestations of IgG4-RD, multimodality imaging features will be discussed, including ultrasound (USG), computed tomography (CT), magnetic resonance imaging (MRI) and 18F-FDG positron emission tomography (PET)-CT.
Key diagnostic clues are highlighted to differentiate IgG4-RD from other malignant conditions through companion case comparison.
Selected cases are also included to demonstrate post-treatment response, in terms of morphological, functional or metabolic assessment with 18F-FDG PET-CT.
PANCREAS AND HEPATOBILIARY SYSTEM
IgG4-related Autoimmune Pancreatitis (AIP)
- Manifests as Type 1 AIP1-2, 7. Not associated with Type 2 AIP1, 7
- Primarily affect middle-aged and elderly men (6th decade)2, 6-7 with higher recurrence rate than Type 2 AIP7
- Associated autoimmune disorders: Sjogren, SLE, primary sclerosing cholangitis (PSC), primary biliary cirrhosis, etc. 10
- Pancreatic morphologic change depends on extent of inflammatory response and fibrosis1, 4
- Diffuse involvement (most common)1-2, 4, 7, 10
- Diffusely enlarged pancreas, loss of normal pancreatic clefts
- Focal lesions1-2, 4, 7, 10
- Mass-like hypoattenuating lesion often at pancreatic head
- Can progress to diffuse involvement4
- USG : Enlarged pancreas with hypoechoic parenchyma6, 10
- CT
- Enhancement reduced in pancreatic phase, near-normal in porto-venous phase1, 6
- Peripancreatic hypoattenuating halo1-2, 5-6
- Minimal peripancreatic fat stranding10
- Rare: Lymphadenopathy, calcifications, and pseudocyst6
- Features favouring AIP over adenocarcinoma7
- Homogeneous enhancement, persistent delayed phase enhancement (c.f. Pancreatic adenocarcinoma minimally enhances1, 7)
- +/- Pancreatic ductal wall enhancement7
- MRI
- T1 hypointense/ T2 hyperintense parenchymal change1, 6-7
- Restricted diffusion1, 7
- Delayed enhancement1, 7
- MR cholangiopancreatography (MRCP)2
- Pancreatic ductal strictures1, 6
- Duct-penetrating sign through AIP involved areas1, 6
- 18F-FDG PET-CT
- Intense FDG tracer uptake of affected segment1, 7
- Usually corticosteroid responsive2, 4, 7, 10
- Improved pancreatic morphology and function within 4-6 weeks2, 6
- Predicting treatment outcome from imaging features4
- Features predicting favourable response: related to early inflammatory changes - Diffuse pancreatic swelling; hypoattenuating halo in CT
- Features predicting suboptimal response: findings that signify fibrosis or late disease stage - Focal mass-like swelling without peripancreatic changes; persistent ductal strictures
Fig 1: IgG4-related autoimmune pancreatitis in 71-year-old woman who presented with epigastric pain and mixed pattern of deranged liver function test. (A) Transabdominal transverse ultrasound (USG) image shows enlarged pancreatic head and proximal body with hypo-echoic echotexture (star). Proximal common bile duct is dilated to 1.1cm (arrow). (B) Axial 18F-FDG PET-CT image shows diffuse sausage-like enlargement of pancreas (loss of lobular contours and pancreatic clefts) (star) with diffusely increased tracer avidity (arrow). No focal lesion detected in pancreas, distal common bile duct and ampulla of Vater. (C) Frontal endoscopic retrograde cholangiopancreatographic (ERCP) image shows lower common bile duct stricture (arrow) with negative cytology for malignancy. Endoscopic ultrasound (not shown) shows diffuse hypo-echoic pancreatic parenchyma with thin rim of peri-pancreatic fluid.
Fig 2: IgG4-related autoimmune pancreatitis in 71-year-old woman who presented with epigastric pain and mixed pattern of deranged liver function test. (A) Transabdominal transverse ultrasound (USG) image shows enlarged pancreatic head and proximal body with hypo-echoic echotexture (star). Proximal common bile duct is dilated to 1.1cm (arrow). (B) Axial 18F-FDG PET-CT image shows diffuse sausage-like enlargement of pancreas (loss of lobular contours and pancreatic clefts) (star) with diffusely increased tracer avidity (arrow). No focal lesion detected in pancreas, distal common bile duct and ampulla of Vater. (C) Frontal endoscopic retrograde cholangiopancreatographic (ERCP) image shows lower common bile duct stricture (arrow) with negative cytology for malignancy. Endoscopic ultrasound (not shown) shows diffuse hypo-echoic pancreatic parenchyma with thin rim of peri-pancreatic fluid.
Fig 3: IgG4-related autoimmune pancreatitis in 71-year-old woman who presented with epigastric pain and mixed pattern of deranged liver function test. (A) Transabdominal transverse ultrasound (USG) image shows enlarged pancreatic head and proximal body with hypo-echoic echotexture (star). Proximal common bile duct is dilated to 1.1cm (arrow). (B) Axial 18F-FDG PET-CT image shows diffuse sausage-like enlargement of pancreas (loss of lobular contours and pancreatic clefts) (star) with diffusely increased tracer avidity (arrow). No focal lesion detected in pancreas, distal common bile duct and ampulla of Vater. (C) Frontal endoscopic retrograde cholangiopancreatographic (ERCP) image shows lower common bile duct stricture (arrow) with negative cytology for malignancy. Endoscopic ultrasound (not shown) shows diffuse hypo-echoic pancreatic parenchyma with thin rim of peri-pancreatic fluid.
Fig 4: Pre- and 5-month Post-treatment axial contrast CT of IgG4-related autoimmune pancreatitis in 76-year-old woman. (A) Pre-treatment axial plain and contrast-enhanced CT shows diffuse enlargement of pancreas with no discrete hypo-enhancing lesion. Note characteristic peripancreatic hypoattenuating halo (arrow). (B) Axial pre-treatment contrast-enhanced CT (left) and follow-up CT 5 months later after corticosteroid administration (right) shows favourable treatment response. Pancreas is no longer swollen (star) with resolved hypoattenuating peripancreatic halo.
Fig 5: Pre- and 5-month Post-treatment axial contrast CT of IgG4-related autoimmune pancreatitis in 76-year-old woman. (A) Pre-treatment axial plain and contrast-enhanced CT shows diffuse enlargement of pancreas with no discrete hypo-enhancing lesion. Note characteristic peripancreatic hypoattenuating halo (arrow). (B) Axial pre-treatment contrast-enhanced CT (left) and follow-up CT 5 months later after corticosteroid administration (right) shows favourable treatment response. Pancreas is no longer swollen (star) with resolved hypoattenuating peripancreatic halo.
Fig 6: Companion case for IgG4-related autoimmune pancreatitis. Exocrine pancreatic adenocarcinoma in a 50-year-old woman who presented with obstructive jaundice. (A) Axial (left) and coronal (right) contrast-enhanced CT shows double duct sign - simultaneously dilated common bile duct (arrow) and pancreatic duct (star), due to malignant biliary obstruction. (B) Follow-up axial plain, axial and coronal contrast-enhanced CT 4 months later clearly shows hypo-vascular nature of tumor with minimal contrast enhancement (arrow).
Fig 7: Companion case for IgG4-related autoimmune pancreatitis. Exocrine pancreatic adenocarcinoma in a 50-year-old woman who presented with obstructive jaundice. (A) Axial (left) and coronal (right) contrast-enhanced CT shows double duct sign - simultaneously dilated common bile duct (arrow) and pancreatic duct (star), due to malignant biliary obstruction. (B) Follow-up axial plain, axial and coronal contrast-enhanced CT 4 months later clearly shows hypo-vascular nature of tumor with minimal contrast enhancement (arrow).
IgG4-related Sclerosing Cholangitis (ISC)
- Second most affected organ after pancreas1-2
- Most frequently affected organ within hepatobiliary system1
- Commonly associated with IgG4-related autoimmune pancreatitis (60 – 80%)1-2, 7
- Diagnostic challenges
- ISC can occur independently without pancreatic involvement1-2, 6
- Overlap with PSC1-2, 6-7, 9 and cholangiocarcinoma2, 9
- ISC typically occur in elderly patient, accompanied by pancreatic or extra-pancreatic lesions, with characteristic long and continuous strictures at ERCP, absent hepatic capsular retraction
- Imaging features
- Thickened bile duct wall with smooth margins1-2, 6-7. Homogeneous enhancement in delayed phase2, 7
- Can affect both intrahepatic and extrahepatic segments of bile ducts causing stenosis and upstream dilatation +/- gallbladder involvement1-2, 6-7
- Most common: common bile duct intrapancreatic portion1, 6
- 18F-FDG PET-CT
- Moderate tracer uptake in involved biliary ducts1
- Usually corticosteroid responsive2, 7, 9
- Biopsy before treatment necessary to exclude potential malignant lesions2
- May experience relapses despite maintenance corticosteroid therapy2
Fig 8: IgG4-related sclerosing cholangitis in a 73-year-old man who presented with tea colour urine and deranged liver function test. (A) Magnetic resonance cholangiopancreatography (MRCP) axial T2 (left) and coronal T2 (right) fat-saturated images show mildly dilated common duct (1cm) (arrow) and prominent intrahepatic ducts (not shown). (B) Similar findings (arrow) are also demonstrated on axial and coronal contrast-enhanced CT images. (C) Coronal MRCP maximum intensity projection (MIP) image (left) and frontal endoscopic retrograde cholangiopancreatographic image (ERCP) (right) shows common bile duct stricture (arrow). Biliary cytology shows cytologic atypia with suspected common duct cholangiocarcinoma. Excision of extrahepatic common bile duct was performed with pathology report revealing IgG4-related sclerosing cholangitis.
Fig 9: IgG4-related sclerosing cholangitis in a 73-year-old man who presented with tea colour urine and deranged liver function test. (A) Magnetic resonance cholangiopancreatography (MRCP) axial T2 (left) and coronal T2 (right) fat-saturated images show mildly dilated common duct (1cm) (arrow) and prominent intrahepatic ducts (not shown). (B) Similar findings (arrow) are also demonstrated on axial and coronal contrast-enhanced CT images. (C) Coronal MRCP maximum intensity projection (MIP) image (left) and frontal endoscopic retrograde cholangiopancreatographic image (ERCP) (right) shows common bile duct stricture (arrow). Biliary cytology shows cytologic atypia with suspected common duct cholangiocarcinoma. Excision of extrahepatic common bile duct was performed with pathology report revealing IgG4-related sclerosing cholangitis.
Fig 10: IgG4-related sclerosing cholangitis in a 73-year-old man who presented with tea colour urine and deranged liver function test. (A) Magnetic resonance cholangiopancreatography (MRCP) axial T2 (left) and coronal T2 (right) fat-saturated images show mildly dilated common duct (1cm) (arrow) and prominent intrahepatic ducts (not shown). (B) Similar findings (arrow) are also demonstrated on axial and coronal contrast-enhanced CT images. (C) Coronal MRCP maximum intensity projection (MIP) image (left) and frontal endoscopic retrograde cholangiopancreatographic image (ERCP) (right) shows common bile duct stricture (arrow). Biliary cytology shows cytologic atypia with suspected common duct cholangiocarcinoma. Excision of extrahepatic common bile duct was performed with pathology report revealing IgG4-related sclerosing cholangitis.
IgG4-related Hepatopathy3, 9, 11
- Hepatic parenchymal disease involvement, manifests as portal inflammation and lobular hepatitis
- Relative new disease entity with limited documentations on pathogenesis and radiological findings
- Can present as infiltrative enhancing mass in periportal location. Potential misdiagnosed as malignant tumour
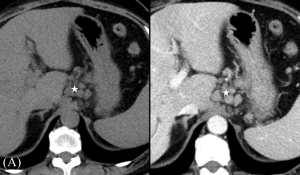
Fig 11: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
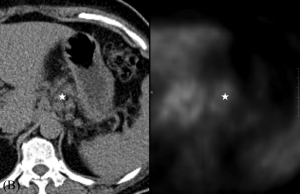
Fig 12: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
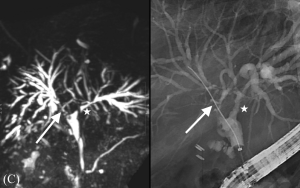
Fig 13: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
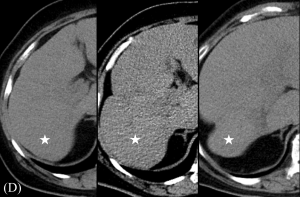
Fig 14: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
MESENTERY AND ALIMENTARY TRACT
IgG4-related Sclerosing Mesenteritis
- Previously considered idiopathic cases are recently recognized as part of IgG4-RD spectrum1
- Characterized by fibrosis and inflammation of mesentery2, 6
- Associated with AIP, ISC, and RPF2
- Imaging features
- Present as soft-tissue mass in small-bowel mesentery, typically located at root and encasing mesenteric vessels1-2, 6
- CT
- Internal calcification is common1
- "Fat ring sign", indicating fibrotic process primarily at the mesentery. Preserved perivascular fat around mesenteric vessels1-2
- Tumoral pseudo-capsule (soft-tissue band at mesenteric borders of mass)1
- Can cause small bowel obstruction due to fibrous tissue mass effect2
- MRI: T1/T2 hypointense mass due to fibrotic tissue1
- 18F-FDG PET-CT: Mild tracer uptake1
- Important differentials to consider1-2
- Carcinoid, lymphoma, mesenteric fibromatosis, carcinomatosis and inflammatory myofibroblastic tumour
Fig 15: IgG4-related sclerosing mesenteritis in 49-year-old female with lower abdominal pain. (A) Axial plain and contrast-enhanced CT shows ill-defined mesenteric soft tissue mass in lower abdomen (star). Note preservation of fat around the superior mesenteric vessels (fat ring sign) (arrow). (B) Axial 18F-FGD PET-CT shows FDG hypermetabolism of mesenteric soft tissue mass (star). No otherwise definite primary site for malignancy identified. (C) Patient was later re-admitted due to abdominal pain and vomiting. Axial (left) and coronal (right) contrast-enhanced CT shows mechanical small bowel obstruction (star) with transition zone at distal ileum, which is infiltrated by soft tissue mass (arrow). Exploratory laparotomy with resection shows IgG4-related sclerosing mesenteritis.
Fig 16: IgG4-related sclerosing mesenteritis in 49-year-old female with lower abdominal pain. (A) Axial plain and contrast-enhanced CT shows ill-defined mesenteric soft tissue mass in lower abdomen (star). Note preservation of fat around the superior mesenteric vessels (fat ring sign) (arrow). (B) Axial 18F-FGD PET-CT shows FDG hypermetabolism of mesenteric soft tissue mass (star). No otherwise definite primary site for malignancy identified. (C) Patient was later re-admitted due to abdominal pain and vomiting. Axial (left) and coronal (right) contrast-enhanced CT shows mechanical small bowel obstruction (star) with transition zone at distal ileum, which is infiltrated by soft tissue mass (arrow). Exploratory laparotomy with resection shows IgG4-related sclerosing mesenteritis.
Fig 17: IgG4-related sclerosing mesenteritis in 49-year-old female with lower abdominal pain. (A) Axial plain and contrast-enhanced CT shows ill-defined mesenteric soft tissue mass in lower abdomen (star). Note preservation of fat around the superior mesenteric vessels (fat ring sign) (arrow). (B) Axial 18F-FGD PET-CT shows FDG hypermetabolism of mesenteric soft tissue mass (star). No otherwise definite primary site for malignancy identified. (C) Patient was later re-admitted due to abdominal pain and vomiting. Axial (left) and coronal (right) contrast-enhanced CT shows mechanical small bowel obstruction (star) with transition zone at distal ileum, which is infiltrated by soft tissue mass (arrow). Exploratory laparotomy with resection shows IgG4-related sclerosing mesenteritis.
IgG4-related Alimentary Tract Sclerosing Disease3, 8, 12
- Relative new disease entity
- Characterized by increased IgG4-positive plasma cell infiltration to glandular tissues or vascular system of gastrointestinal tract, resulting in ulcers, polypoid lesions, submucosal masses and wall thickening
- Radiological features : Submucosal oedema, mural thickening of affected bowel segment, mimic malignancy

Fig 18: IgG4-related alimentary tract sclerosing disease in 64-year-old man who presented with tender right lower abdomen mass and one-week history of absent bowel opening. (A) Axial (left) and coronal (right) contrast-enhanced CT shows significant mural thickening at terminal ileum, right sided colon involving cecum and ascending colon, with content stasis in upstream small bowel leading to small bowel faeces sign at distal ileum (arrow). Intestines are otherwise not dilated. Right hemicolectomy with end-to-end ileocolic anastomosis performed with tumour suspicion. Intra-operative finding of 5cm caecal mass with adhesion to terminal ileum and retroperitoneum. Pathology confirms IgG4-related sclerosing disease. (B) Axial plain and contrast-enhanced CT status 1-month post-operation shows ileocolic anastomotic leakage with extra-luminal gas (arrow) and fluid. Intra-operative finding of 1cm dehiscence at anastomosis with small bowel resection and exteriorization performed. Pathology reveals IgG4-related disease infiltration to anastomosis.
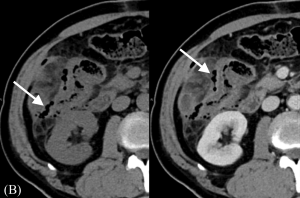
Fig 19: IgG4-related alimentary tract sclerosing disease in 64-year-old man who presented with tender right lower abdomen mass and one-week history of absent bowel opening. (A) Axial (left) and coronal (right) contrast-enhanced CT shows significant mural thickening at terminal ileum, right sided colon involving cecum and ascending colon, with content stasis in upstream small bowel leading to small bowel faeces sign at distal ileum (arrow). Intestines are otherwise not dilated. Right hemicolectomy with end-to-end ileocolic anastomosis performed with tumour suspicion. Intra-operative finding of 5cm caecal mass with adhesion to terminal ileum and retroperitoneum. Pathology confirms IgG4-related sclerosing disease. (B) Axial plain and contrast-enhanced CT status 1-month post-operation shows ileocolic anastomotic leakage with extra-luminal gas (arrow) and fluid. Intra-operative finding of 1cm dehiscence at anastomosis with small bowel resection and exteriorization performed. Pathology reveals IgG4-related disease infiltration to anastomosis.
GENITOURINARY SYSTEM AND RETROPERITONEUM
IgG4-related Renal Disease
- Kidney: Most frequently involved genitourinary organ5
- More commonly manifested as tubulointerstitial nephritis than membranous glomerulonephropathy1, 5
- Obstructive nephropathy possible due to post-renal obstruction1-2, 5-7
- Commonly presented as acute or progressive renal failure1
- Prompt diagnosis and treatment to prevent chronic kidney disease1. Usually corticosteroid responsive2, 5, 7
- Tubulointerstitial Nephritis classified into
- Parenchymal involvement (most common)
- CT: Present as small round or wedge-shaped peripheral hypo-enhancing cortical lesions1-2, 5, 7
- Differentials: Multifocal pyelonephritis, metastasis, lymphoma2, 5, 7
- MRI: T1/T2 hypointense. Gradual progressive enhancement, +/- diffusion restriction1-2, 5, 7
- Renal pelvic involvement
- Present as masses in renal pelvis or diffuse pelvic wall thickening1, 5, 7
- Mimic renal cell carcinoma and urothelial cell carcinoma5
- Perinephric involvement
- Present as a diffuse rind of soft tissue surrounding the kidney1, 5, 7
- Excretory phase CT urography may show extrinsically compressed collecting systems1-2, 5-7 without intraluminal defect, aiding differentiation from urothelial tumours
- 18F-FDG PET-CT
- Limited use for initial evaluation due to physiologic renal radiotracer excretion1
- Monitor treatment response in known cases to guide treatment duration5
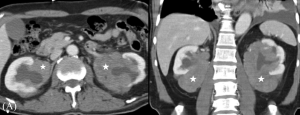
Fig 20: IgG4-related renal pelvic disease in a 72-year-old man. Tapering of immunosuppressive therapy based on FDG inactivity and lack of active inflammation on repeat biopsy post-treatment. (A) Pre-treatment axial (left) and coronal (right) contrast-enhanced CT image at presentation shows ill-defined mildly enhancing soft tissue mass (star) encasing renal pelvises or sinuses, causing hydronephroses. (B) Post-treatment axial contrast-enhanced CT 5 years later shows partial resolution of bilateral peri-pelvic soft tissue lesions with residue (arrows). (C) Subsequent 18F-FDG PET-CT shows no significant FDG metabolism of soft tissue lesion (star). Biopsy of the lesion shows fibrous tissue with no significant inflammation. In view of inactive disease with predominant fibrosis, immunosuppressive treatment was gradually tapered down. (D) Another similar biopsy-proven case of IgG4-related renal pelvic disease. Excretory phase of coronal maximum intensity projection (MIP) (left) and axial (right) images of contrast-enhanced CT Urography shows soft tissue thickening with smooth outer border, encasing left renal pelvis (arrow). Note the compressed upper collecting system also retains smooth inner surface with no discrete intra-luminal filling defect, rendering urothelial tumour origin unlikely.
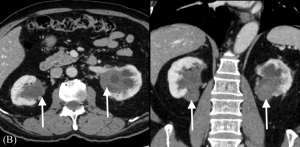
Fig 21: IgG4-related renal pelvic disease in a 72-year-old man. Tapering of immunosuppressive therapy based on FDG inactivity and lack of active inflammation on repeat biopsy post-treatment. (A) Pre-treatment axial (left) and coronal (right) contrast-enhanced CT image at presentation shows ill-defined mildly enhancing soft tissue mass (star) encasing renal pelvises or sinuses, causing hydronephroses. (B) Post-treatment axial contrast-enhanced CT 5 years later shows partial resolution of bilateral peri-pelvic soft tissue lesions with residue (arrows). (C) Subsequent 18F-FDG PET-CT shows no significant FDG metabolism of soft tissue lesion (star). Biopsy of the lesion shows fibrous tissue with no significant inflammation. In view of inactive disease with predominant fibrosis, immunosuppressive treatment was gradually tapered down. (D) Another similar biopsy-proven case of IgG4-related renal pelvic disease. Excretory phase of coronal maximum intensity projection (MIP) (left) and axial (right) images of contrast-enhanced CT Urography shows soft tissue thickening with smooth outer border, encasing left renal pelvis (arrow). Note the compressed upper collecting system also retains smooth inner surface with no discrete intra-luminal filling defect, rendering urothelial tumour origin unlikely.
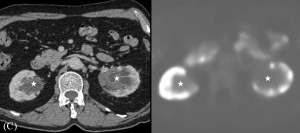
Fig 22: IgG4-related renal pelvic disease in a 72-year-old man. Tapering of immunosuppressive therapy based on FDG inactivity and lack of active inflammation on repeat biopsy post-treatment. (A) Pre-treatment axial (left) and coronal (right) contrast-enhanced CT image at presentation shows ill-defined mildly enhancing soft tissue mass (star) encasing renal pelvises or sinuses, causing hydronephroses. (B) Post-treatment axial contrast-enhanced CT 5 years later shows partial resolution of bilateral peri-pelvic soft tissue lesions with residue (arrows). (C) Subsequent 18F-FDG PET-CT shows no significant FDG metabolism of soft tissue lesion (star). Biopsy of the lesion shows fibrous tissue with no significant inflammation. In view of inactive disease with predominant fibrosis, immunosuppressive treatment was gradually tapered down. (D) Another similar biopsy-proven case of IgG4-related renal pelvic disease. Excretory phase of coronal maximum intensity projection (MIP) (left) and axial (right) images of contrast-enhanced CT Urography shows soft tissue thickening with smooth outer border, encasing left renal pelvis (arrow). Note the compressed upper collecting system also retains smooth inner surface with no discrete intra-luminal filling defect, rendering urothelial tumour origin unlikely.
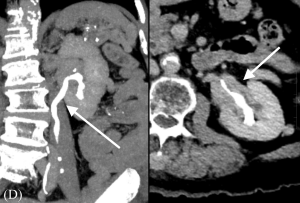
Fig 23: IgG4-related renal pelvic disease in a 72-year-old man. Tapering of immunosuppressive therapy based on FDG inactivity and lack of active inflammation on repeat biopsy post-treatment. (A) Pre-treatment axial (left) and coronal (right) contrast-enhanced CT image at presentation shows ill-defined mildly enhancing soft tissue mass (star) encasing renal pelvises or sinuses, causing hydronephroses. (B) Post-treatment axial contrast-enhanced CT 5 years later shows partial resolution of bilateral peri-pelvic soft tissue lesions with residue (arrows). (C) Subsequent 18F-FDG PET-CT shows no significant FDG metabolism of soft tissue lesion (star). Biopsy of the lesion shows fibrous tissue with no significant inflammation. In view of inactive disease with predominant fibrosis, immunosuppressive treatment was gradually tapered down. (D) Another similar biopsy-proven case of IgG4-related renal pelvic disease. Excretory phase of coronal maximum intensity projection (MIP) (left) and axial (right) images of contrast-enhanced CT Urography shows soft tissue thickening with smooth outer border, encasing left renal pelvis (arrow). Note the compressed upper collecting system also retains smooth inner surface with no discrete intra-luminal filling defect, rendering urothelial tumour origin unlikely.
Fig 24: Companion case for IgG4-related renal pelvic disease. Incidental finding of B-cell right renal sinus lymphoma in a hepatitis-B infected 52-year-old man who underwent routine screening for hepatocellular carcinoma. Axial plain and contrast-enhanced CT shows abnormal enhancing soft tissue lesion with ill-defined infiltrative border that involves the right renal sinus (arrow) and upper ureter (not shown). Subsequent biopsy showed extra-nodal marginal zone B-cell lymphoma of MALT type.
IgG4-related Retroperitoneal Fibrosis (RPF)
- Chronic inflammation with IgG4-positive plasma cells retroperitoneal infiltration, leading to fibrotic tissue formation around infra-renal abdominal aorta, commonly extending to iliac vessels1-2, 5-7
- Entrapped ureters resulting in obstructive uropathy1-2, 5-7
- Imaging features
- Soft tissue lesion hypoechoic on USG, homogenously attenuating on CT, T1 hypointense/variable T2 signal intensity on MRI depending on inflammation and fibrosis1, 5-7
- Enhancement pattern on CT and MRI indicate disease activity and treatment response1, 5-6
- Active inflammatory RPF: Early enhancement
- Chronic non-active RPF: Delayed enhancement
- 18F-FDG PET-CT
- Assess disease activity and residual disease1,5,7
- Predict treatment prognosis1
- Important differentials to consider1-2, 5
- Lymphoma, large-vessel vasculitis (e.g. giant cell arteritis or Takayasu arteritis), aortitis associated with syphilis or sarcoidosis
- Usually corticosteroid responsive6-7
Fig 25: IgG4-related retroperitoneal fibrosis in 75-year-old man who presented with acute on chronic renal failure. (A) Axial 18F-FDG PET-CT shows FDG-avid retroperitoneal soft tissue lesion infiltrating left renal hilum (star), right ureter (not shown) and encasing abdominal aorta (arrow). Upstream obstructive uropathy with bilateral hydronephroses are seen, worse on right. (B) MR Urography axial T1 (upper left) and axial T2 (upper right) images show heterogenous intermediate T1 and low T2 signal retroperitoneal soft tissue (arrow). Coronal T2 (lower left) and Maximum intensity projection (MIP) images (lower right) demonstrates bilateral hydronephroses with tapering at upper ureters, in keeping with urinary obstruction due to bilateral ureteric encasement by retroperitoneal tissues. (C) Subsequent CT-guided percutaneous biopsy confirms IgG4-related retroperitoneal fibrosis.
Fig 26: IgG4-related retroperitoneal fibrosis in 75-year-old man who presented with acute on chronic renal failure. (A) Axial 18F-FDG PET-CT shows FDG-avid retroperitoneal soft tissue lesion infiltrating left renal hilum (star), right ureter (not shown) and encasing abdominal aorta (arrow). Upstream obstructive uropathy with bilateral hydronephroses are seen, worse on right. (B) MR Urography axial T1 (upper left) and axial T2 (upper right) images show heterogenous intermediate T1 and low T2 signal retroperitoneal soft tissue (arrow). Coronal T2 (lower left) and Maximum intensity projection (MIP) images (lower right) demonstrates bilateral hydronephroses with tapering at upper ureters, in keeping with urinary obstruction due to bilateral ureteric encasement by retroperitoneal tissues. (C) Subsequent CT-guided percutaneous biopsy confirms IgG4-related retroperitoneal fibrosis.
Fig 27: IgG4-related retroperitoneal fibrosis in 75-year-old man who presented with acute on chronic renal failure. (A) Axial 18F-FDG PET-CT shows FDG-avid retroperitoneal soft tissue lesion infiltrating left renal hilum (star), right ureter (not shown) and encasing abdominal aorta (arrow). Upstream obstructive uropathy with bilateral hydronephroses are seen, worse on right. (B) MR Urography axial T1 (upper left) and axial T2 (upper right) images show heterogenous intermediate T1 and low T2 signal retroperitoneal soft tissue (arrow). Coronal T2 (lower left) and Maximum intensity projection (MIP) images (lower right) demonstrates bilateral hydronephroses with tapering at upper ureters, in keeping with urinary obstruction due to bilateral ureteric encasement by retroperitoneal tissues. (C) Subsequent CT-guided percutaneous biopsy confirms IgG4-related retroperitoneal fibrosis.
IgG4-related Aortitis
- More common in adult male13
- Presents as non-stenotic aortic mass with thickened aortic walls and irregular margins1-2,7
- Typically associated with IgG4-related retroperitoneal fibrosis13
- Progress to aortic aneurysm formation1-2, 7, 13
- Risk of rupture lower than other inflammatory diseases1
- CT
- Homogeneous late enhancement of aortic mass1-2, 7, 13
- Other organ involvement is common13
- MRI
- Low to intermediate T1/ variable T2 signal intensity in aortic mass1
- 18F-FDG PET-CT
- Moderate to intense tracer uptake in mass1,7
- Important differential to consider: Lymphoma13
- Clue: Presence of IgG4-RD in other organs and IgG4 serologic examination
- Usually corticosteroid responsive13
- Steroid therapy may increase rupture risk in aneurysmal IgG4-related peri-aortitis, by promoting arterial wall thinning13
Fig 28: IgG4-related aortitis in 64-year-old man who presented with abdominal pain and vomiting. (A) Axial (left) and coronal (right) contrast-enhanced CT image shows circumferential thickening of aortic wall (star) with peri-aortic soft tissue extending to common iliac arteries (arrow). (B) Axial 18F-FDG PET-CT image shows ring of hypermetabolic soft tissue encasing abdominal aorta (arrow). Note smooth outline of soft tissue lesion, in contrast to lobulated nodular contour more commonly seen in retroperitoneal tumours. (C) Comparison of CT at presentation (left) and 4 years after (right) shows interval shrinkage of periaortic soft tissue infiltrate (arrow) , with residual chronic thickening due to multiple disease flares.
Fig 29: IgG4-related aortitis in 64-year-old man who presented with abdominal pain and vomiting. (A) Axial (left) and coronal (right) contrast-enhanced CT image shows circumferential thickening of aortic wall (star) with peri-aortic soft tissue extending to common iliac arteries (arrow). (B) Axial 18F-FDG PET-CT image shows ring of hypermetabolic soft tissue encasing abdominal aorta (arrow). Note smooth outline of soft tissue lesion, in contrast to lobulated nodular contour more commonly seen in retroperitoneal tumours. (C) Comparison of CT at presentation (left) and 4 years after (right) shows interval shrinkage of peri-aortic soft tissue infiltrate (arrow) , with residual chronic thickening due to multiple disease flares.
Fig 30: IgG4-related aortitis in 64-year-old man who presented with abdominal pain and vomiting. (A) Axial (left) and coronal (right) contrast-enhanced CT image shows circumferential thickening of aortic wall (star) with peri-aortic soft tissue extending to common iliac arteries (arrow). (B) Axial 18F-FDG PET-CT image shows ring of hypermetabolic soft tissue encasing abdominal aorta (arrow). Note smooth outline of soft tissue lesion, in contrast to lobulated nodular contour more commonly seen in retroperitoneal tumours. (C) Comparison of CT at presentation (left) and 4 years after (right) shows interval shrinkage of peri-aortic soft tissue infiltrate (arrow) , with residual chronic thickening due to multiple disease flares.
LYMPHATIC SYSTEM
IgG4-related Lymphadenopathy
- Non-specific early sign of IgG4-RD; often recognized after other organ involvement1-2
- Most common affecting mediastinal and abdominal (especially peripancreatic, periportal and para-aortic) nodes1-2, 6
- Next cervical, axillary, and pulmonary hilar nodes1-2, 6
- Smaller lymph nodes (<2 cm) compared to other diseases, e.g. lymphoma and Castleman disease, and absent systemic symptoms (fever, weight loss)1-2, 6
- Imaging features non-specific
- USG: Initial imaging modality, diffuse nodal cortical thickening with fatty hilum preservation1
- 18F-FDG PET-CT: Avid tracer uptake in affected lymph node1
- Usually corticosteroid responsive6
Fig 11: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
Fig 12: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
Fig 13: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.
Fig 14: IgG4-related lymphadenopathy in a 57-year-old woman who presented with deranged liver function test, with subsequent development of IgG4-related sclerosing cholangitis and hepatopathy. (A) Axial plain and contrast-enhanced CT image demonstrates clusters of multiple portal, para-aortic and gastro-hepatic lymphadenopathy (star). Mildly prominent intrahepatic ducts seen (not shown). (B) Axial 18F-FDG PET-CT shows FDG-avidity of the lymph nodes (star), with no suspicious adjacent primary tumour. Endoscopic ultrasound guided biopsy of lymph node confirms the diagnosis of IgG4-related lymphadenopathy. Concurrent biopsy of liver shows chronic cholangitis with no evidence of primary sclerosing cholangitis, primary biliary cirrhosis or IgG4-related cholangitis. Patient was treated with corticosteroid and subsequent liver function test normalized. (C) Interval follow-up and laboratory tests revealed acutely deranged liver function. MR cholangiogram (left) and ERCP (right) shows mildly dilated bilateral intrahepatic ducts with focal irregular tapering (star) towards porta hepatis. Right intrahepatic duct stricture also seen in ERCP (arrow). Histology studies revealed IgG4-related sclerosing cholangitis. (D) Serial axial plain CTs at presentation (left), 2 years (middle) and 3 years (right) after diagnosis of IgG4-related sclerosing cholangitis, shows progressive right hepatic lobe atrophy with widened fissure (star). USG-guided biopsy of right hepatic lobe shows IgG4-related hepatopathy.




















