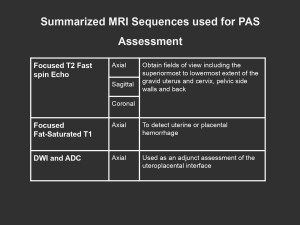
This exhibit employs a retrospective analysis of the MRI scans done at our institution for evaluating PAS disorders and their associated imaging findings. We utilize 1.5 and 3.0 Tesla scanners with a multichannel, phased-array surface coil. Overall, 3.0 Tesla MRI provides greater signal intensity and spatial resolution, allowing for evaluation of smaller details which may better delineate the uteroplacental interface for the evaluation of foci of invasion. Key sequences are detailed in Figure 2.
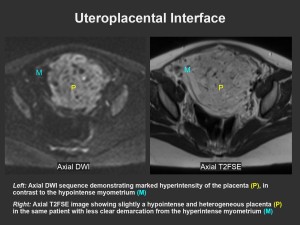
DWI can be used to delineate placenta from myometrium in cases where both show similar signals on T2
Normal Placenta and Myometrium on MRI
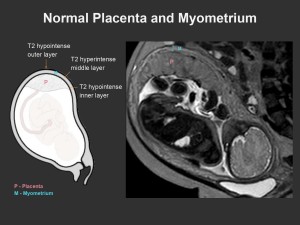
The normal placenta is discoid in morphology with smooth uniform contours and homogeneous moderate T2-hyperintensity relative to the myometrium. Thin T2-hypointense septa are often seen coursing through the placenta, surrounding placental cotyledons. As the placenta matures, it may demonstrate mild lobulation and heterogeneity. The placenta is increasingly “consumed” during late gestation resulting in signal changes reflecting decreased tissue density, areas of calcification, and infarction. Placental infarcts are found in approximately 25% of uncomplicated term pregnancies[3]. These processes may mimic heterogeneous signals seen in PAS disorders. Therefore, the optimal time for performing MRI is between 28 and 32 weeks[4].
The myometrium adjacent to the placenta normally exhibits a trilaminar appearance: T2-hypointense outer serosal layer, T2-hyperintense to intermediate middle layer, and T2-hypointense inner layer (i.e. uteroplacental interface). Few vascular flow voids may be seen in the middle layer. Late in gestation, the trilaminar appearance may be lost resulting in a single T2-hypointense line, with compression of the middle layer[2]. The uterine morphology should remain an inverted pear shape, with the fundus larger than the lower uterine segment. Myometrial contractions in normal pregnancy represent a potential pitfall. These appear as focal T2-hypointense thickening and distortion of the myometrium which should resolve in subsequent sequences.
Figure 4 shows the normal appearance of the placenta and adjacent myometrium on MRI.
“UTERINE” Approach to MRI Findings in Placenta Accreta Spectrum
We suggest using the acronym “UTERINE” to recall the seven recommended MRI features of PAS disorders in the 2020 Society of Abdominal Radiology (SAR) and European Society of Urogenital Radiology (ESUR) joint consensus statement:
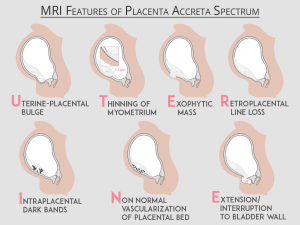
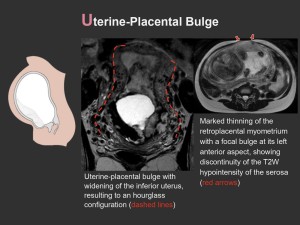
(U)terine-Placental Bulge
- Focal bulge of the uterine contour or a lower uterine segment wider than the fundus = hourglass-shaped uterus
- Uterine-placental bulge with other features of PAS is 100% predictive of myometrial invasion, i.e. increta and percreta[2]
- If alone, can lead to false-positive results
- Myometrial vascular congestion can complicate delineation of the placental contour
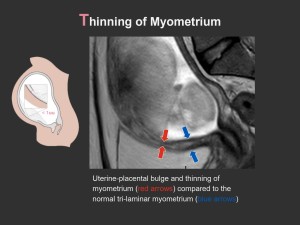
(T)hinning of Myometrium
- Myometrial thinning to less than 1 mm or invisible
- May be loss of the placental trilaminar appearance late in gestation but the T2-hypointense serosal margin should remain intact
- Nonpathologic myometrial thinning may be seen in areas of myometrial compression (e.g. between the uterus and the maternal spine)
(E)xophytic Mass (Focal)
- Placental tissue seen protruding through the uterine wall
- Highly specific for placenta percreta
- Absent in placenta accreta or increta

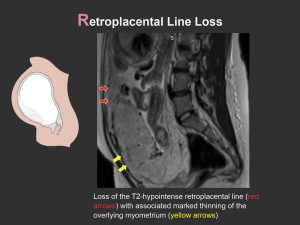
(R)etroplacental Line Loss
- Focal interruption or diffuse loss of the thin T2-hypointense uteroplacental interface
- Combined with focal myometrial defects/thinning, it can be highly sensitive (97%) and predictive of PAS but poorly specific (36%)[4]
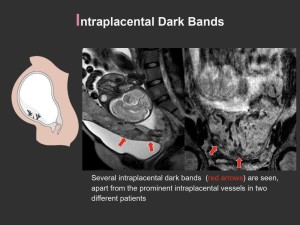
(I)ntraplacental Dark Bands
- Thick (6 to 20 mm), irregular T2 dark bands representing fibrin deposition from hemorrhage and infarcts, contrary to the thin septa seen in a normal placenta
- Most sensitive (80-90%) MRI feature for PAS disorders, with moderate specificity (50-60%)[2]
- Contributes to heterogeneous appearance of the placenta
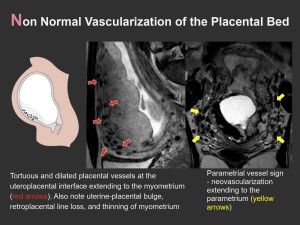
(N)on Normal Vascularization of the Placental Bed
- Disrupted vascular architecture with prominent vessels in the placental bed and disruption of the uteroplacental interface, which may extend to the myometrium
- Neovascularization extending to the vesicouterine space (“bladder vessel” sign) or to the parametrium (“parametrial vessel” sign)
- Significant prognostic factor discriminating between placenta percreta and accreta/increta
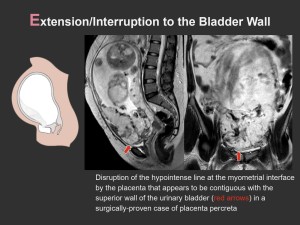
(E)xtension/Interruption to the Bladder Wall
- Interruption, irregularity, or “tenting” of the bladder wall
- Placental tissue in the bladder lumen is highly specific (100%) but is not common
Other features categorized as “uncertain” in the 2020 SAR-ESUR consensus statement include placental heterogeneity, asymmetric thickening/shape of the placenta, placental ischemic infarction, and abnormal intraplacental vascularity.
Evaluating for Myoinvasion
On MRI, PAS disorders may be characterized as accreta/increta versus percreta based on depth of invasion. Determining the presence or absence of myometrial invasion may be challenging. In general, distinguishing between placenta accreta and increta is unnecessary as it will not significantly alter the treatment plan[5]. On the other hand, diagnosis of percreta will alter the management. Definitive diagnosis of percreta requires features such as full thickness gap of myometrial signal with loss of fat plane between the placental tissue and adjacent pelvic organs and intermediate placental signal disrupting the hypointense line of the bladder, bowel wall, or abdominopelvic wall muscles. Other features that have been associated with a higher likelihood of percreta include higher volume of intraplacental dark bands, greater uterine-placental bulge, and marked uteroplacental hypervascularity[2]. A meta-analysis by Familiari et al. found that the diagnostic accuracy of MRI in detecting the depth of placental invasion is similar to ultrasound[6].
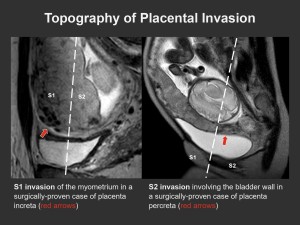
The topography of placental invasion can help in deciding the best approach for treatment. Surgical treatment revolves around controlling the vascular supply of aberrant placental tissue, thus surgeons determine the topography of placental invasion by drawing a line perpendicular from the midline posterior urinary bladder wall, dividing the uterus into two regions. The upper upper area is named S1, corresponding to the uterine fundus and body while the area below this line is named S2, which corresponds to the lower uterus, cervix, and upper vagina (Figure 13). The anterior peritoneal reflection which is located at the level of the cervico-uterine junction is a more concrete landmark delineating the two areas[4]. For S1 invasions, controlling the ovarian and uterine arteries (branches of the anterior internal iliac artery and infrarenal abdominal aorta) proves effective. For S2 invasions, vascular control is more complicated as it involves treating the various anastomotic systems including the vesicouterine, vesicoplacental, and colpouterine systems[7]. Higher maternal maternal morbidity is thus associated with S2 invasion[2].