
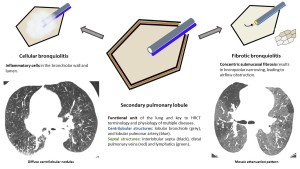
Even though there is no consensus classification system for small airways disease, one of the most accepted and used at pathologic examinations divides these conditions into two broad categories: cellular bronchiolitis (CB) and constrictive or fibrotic bronchiolitis (FB).
Histologically, CB is characterized by inflammatory cells as the predominant feature, in contrast to FB, which refers to bronchiolar narrowing due to adventitial and submucosal fibrosis.
Various forms of CB are well acknowledged, encompassing infectious bronchiolitis (IB), respiratory bronchiolitis (RB), aspiration bronchiolitis (AB), follicular bronchiolitis (FLB), hypersensitivity pneumonitis (HP), and diffuse panbronchiolitis (DP).
On the contrary, although FB can occur in isolation, it is typically a pathologic pattern resulting from other conditions (eg, chronic rejection in the setting of transplantation, an infection, or an autoimmune process).
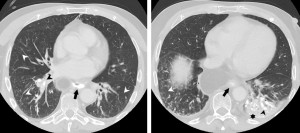
Chest radiographs are frequently normal in small airways diseases, however, they may manifest with nonspecific findings such as ill-defined small or hazy clustered nodules (fig.3) in CB or areas of air trapping characterized by hyperlucency in FB (fig.4).


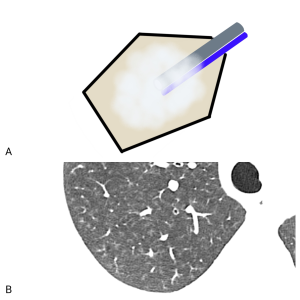
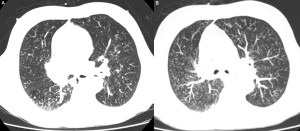
At chest CT, the primary manifestation of CB is centrilobular nodules (fig.5). These nodules can vary in size and attenuation. If they coalesce, may form nodular foci of consolidation or ground-glass opacities (fig.6).
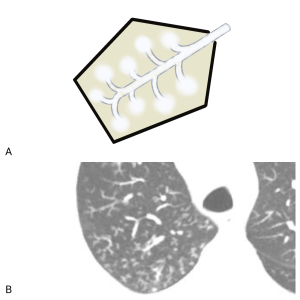
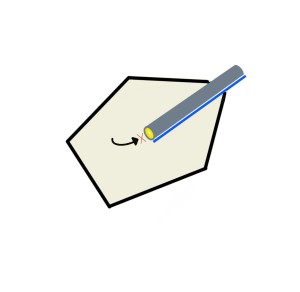
The other important manifestation of CB is the tree-in-bud pattern, which refers to a specific subset of centrilobular nodules with multiple, branching, soft tissue attenuation opacities originating from a single stalk (fig.7).
Different conditions beneath CB exhibit overlapping appearances on chest CT. However, some findings may assist in refining the differential diagnosis, in addition to using clinical information. The tree-in-bud pattern is commonly associated with IB or AB, while isolated centrilobular nodules tend to indicate conditions such as HP or RB.
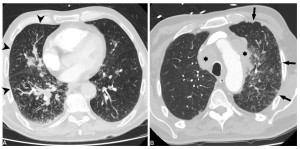
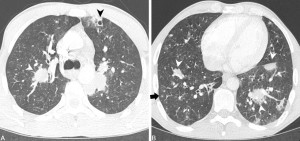
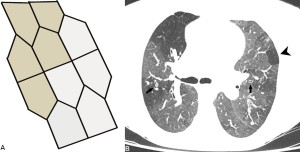
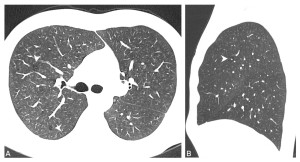
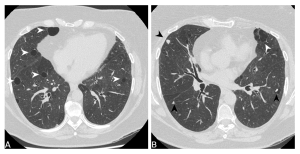
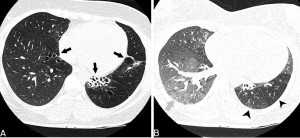
A pivotal aspect of bronchiolitis assessment involves ensuring that micronodules are accurately identified as centrilobular rather than perilymphatic. This distinction is based on their anatomic distribution. Centilobular nodules are defined by their limited extent, not reaching the pleura or fissures (fig.8A-9A). In contrast, perilymphatic micronodules typically engage the pleural surfaces and fissures (fig.8B-9B).
Once micronodules are established as centrilobular, it becomes crucial to ascertain their association with small airways disease and exclude vascular causes, since the other centrilobular structure is the lobular pulmonary artery. While these micronodules may be indistinguishable from those observed in bronchiolitis, they tend to be diffusely distributed throughout the lungs, stemming from hematogenous dissemination of disease and they often associate key ancillary findings (fig.10).
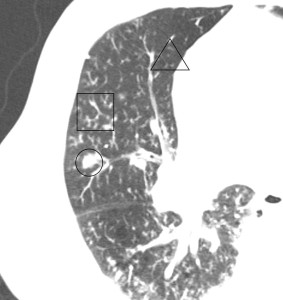
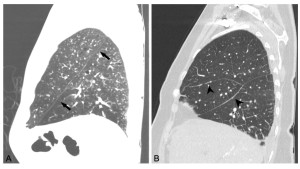
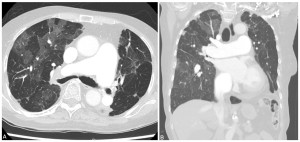
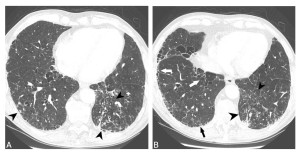
FB frequently manifests as mosaic attenuation due to air trapping caused by bronchiolar narrowing (fig.11).
This air trapping typically exhibits sharply delineated borders where the abnormal SPLs interface with the normal ones (fig.12). Concurrent findings include bronchial wall thickening (fig.12B) and bronchiectasis.
Mosaic attenuation is not always attributable to bronchiolitis. Chronic vascular diseases may manifest as mosaic attenuation on imaging. Distinguishing between airway and vascular mosaic attenuation poses challenges, but the identification of ancillary findings proves helpful, as the evidence of pulmonary hypertension or nonocclusive eccentric pulmonary artery filling defects (fig.13).
We provide a summary of SPL, CB and FB and their pathological findings with radiological correlation in fig.14.
After reviewing the two broad categories of bronchiolitis and their associated radiological findings, next-step involves describing the various small airways diseases, starting with those included in cellular bronchiolitis.
Infectious bronchiolitis
The most common type of bronchiolitis. It can be classified as either acute (typically viral) or chronic (frequently mycobacterial or bacterial). Acute infection often manifests with scattered foci of clustered tree-in-bud opacities and bronchial wall thickening (fig.15). Chronic infectious bronchiolitis may associate other imaging findings beyond tree-in-bud opacities that indicate chronicity such as bronchiectasis (fig.16).

Clinical manifestations include include fever, dyspnea, productive cough, and wheezing.
Aspiration bronchiolitis
The second most common type of bronchiolitis and often misdiagnosed as IB. Many clinical conditions increase the risk of aspiration, including altered mental status, neurological disorders, head and neck cancer or irradiation, as well as esophageal and gastric abnormalities.
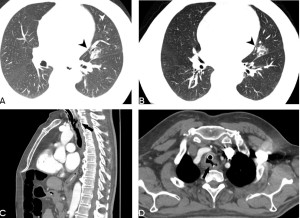
On imaging, it typically presents with tree-in-bud opacities sometimes accompanied by bronchocentric consolidation (fig.17A-B, fig.18B). Radiologists should strive to identify associated conditions to establish a connection between bronchiolitis and aspiration (fig.17C-D, fig.18).
Respiratory bronchiolitis
RB almost always occurs in smokers and is considered part of the spectrum that includes desquamative interstitial pneumonia.
On imaging, it typically presents upper lobe-predominant centrilobular nodules, often associated with other smoking-related lung diseases, such as emphysema (fig.19).
Hypersensitivity pneumonitis
HP is an allergic lung disease caused by inhalational exposure to numerous offending agents. This condition presents a wide spectrum of signs and symptoms, with the key challenge being identifying the antigen exposure.
Active HP often manifests with diffuse or lower lobe-predominance (fig.20), symmetric, poorly defined centrilobular nodules or groud-glass opacities (fig.21A). Air trapping is not uncommon and can serve as a valuable distinguishing factor between HP and other conditions featuring ground-glass centrilobular nodules. It also indicates a component of FB (fig.21B).


Follicular bronchiolitis
FLB represents peribronchiolar lymphoid hyperplasia along the small airways. It typically presents centrilobular nodules corresponding to nodular lymphoid aggregates (fig.22). FLB is part of a spectrum of lymphoproliferative lung disorders of the lung, which includes lymphoid interstitial pneumonia (fig.23).
FB usually occurs in middle-aged adults with progressive cough and dyspnea and underlying immunodeficiency.
Diffuse panbronchiolitis
DP is the rarest form of CB and predominantly affects middle-aged Japanese men. The etiology remains unknown.
DP often involves both upper and lower respiratory systems. On imaging, it typically presents with lower lobe-predominant centrilobular nodules and tree-in-bud opacities, which may progress to brochiolectasis and bronchiectasis. Additionally, mosaic attenuation and the presence of cystic spaces are indicative of FB.
Fibrotic bronchiolitis
Constrictive or fibrotic bronchiolitis refers to bronchiolar narrowing resulting from irreversible concentric submucosal fibrosis, leading to airflow obstruction and subsequent mosaic attenuation pattern.
FB represents a pattern of lung response to a variety of insults. The most relevant etiologies include:
Childhood infection: Swyer-Javes-MacLeod syndrome represents a post-infectious FB that involves the lungs in a non-uniform manner (fig.24).
Transplant-related: Bronchiolitis obliterans syndrome is a well-known complication occurring at least 3 months after lung transplantation. It is also common in graft-versus-host disease associated with hematopoietic stem cell transplantation.
Inhalational lung disease: Various inhalational exposures have been implicated in the development of FB.
Connective tissue disease: FB has been described in connective tissue diseases, most commonly observed in women with advanced rheumatoid arthritis (fig.25).

Some etiologies described in CB (as HP or DP) may manifest FB findings.