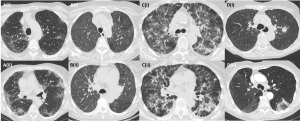
The incidence of DILD is on the rise, especially with the introduction of new targeted drugs which may yield pulmonary side effects, and it is now estimated to be around 12 cases per million individuals/year. The main drugs related to DILD listed according to prevalence are chemotherapeutic or immunotherapeutic agents, anti-inflammatory medications, cardiovascular agents, and antibiotics. DILD can have an acute and severe, or chronic and more insidious presentation of symptoms which are often non-specific. The main pathological patterns are of diffuse alveolar damage, eosinophilic pneumonia, hypersensitivity pneumonitis, organising pneumonia (OP), sarcoid-like reaction, and fibrosis, usually with non-specific interstitial pneumonitis (NSIP) pattern. The main issue with diagnosing DILD stems from the fact that pulmonary toxicity has been described for a wide variety of substances, accounting from 3-5% of all cases of ILD, with a variable time interval between drug administration and onset of DILD [1]. Moreover, different drugs may cause the same imaging patterns of DILD, and the same drugs may cause different pathological patterns (Fig.1). Clinical symptoms, imaging and serology are not specific for DILD, and patients often have multiple comorbidities or risk factors for developing underlying lung disease that can cause the same imaging appearances as a drug reaction. If unrecognised and untreated, DILD may yield severe consequences, such as non-reversible fibrosis and loss of lung function [2, 3]. As such, it is important that radiologists are aware of the medications associated with DILD from different clinical settings (such as gastroenterology or rheumatology clinics).