Introduction
Primary retroperitoneal masses constitute a rare group of lesions which do not originate from a specific retroperitoneal organ. Majority of these mass lesions are malignant (~ 70-80%) and are associated with high mortality rates owing to non specific clinical features and late presentation. Determining the anatomic extent and key imaging features of primary retroperitoneal masses is crucial for providing an accurate diagnosis and in selecting the appropriate clinical management. By early detection and proper evaluation of retroperitoneal masses through cross sectional imaging modalities, the radiologist can aid in early treatment and thus ensure better prognosis.
Anatomy of the retroperitoneal spaces
The retroperitoneum is a compartmentalized extraperitoneal space that extends from the diaphragm superiorly to the pelvis inferiorly, and is situated between the posterior parietal peritoneum anteriorly and the transversal fascia posteriorly.
It is divided into 3 compartments by well-defined fascial planes: anterior renal fascia, posterior renal fascia, and lateroconal fascia
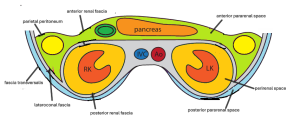
Compartments
- Anterior Pararenal Space
Limits:
- Anterior: parietal peritoneum
- Posterior: anterior renal fascia
- Laterally: lateroconal fascia.
Content: ascending and descending colon, duodenum, pancreas.
- Perirenal Space
Limits:
- Anterior: anterior renal fascia
- Posterior: posterior renal fascia
- The renal fascia joins and closes the perirenal space resembling an inverted cone with its tip in the iliac fossa.
Content: kidneys, adrenal glands, ureters.
- Posterior pararenal space
Limits:
- Anterior: posterior renal fascia
- Posterior: fascia transversalis.
Content: fat.
- The great vessel compartment
Limits:
- between perirenal spaces;
- Anterior: the anterior perirenal space;
- Posterior: the spine, extending from T12 to L5.
Contents: abdominal aorta and its branches, inferior vena cava and its tributaries; lymphatic chains; abdominal sympathetic trunk.
Before assessing the specific imaging characteristics of retroperitoneal masses, it is important to first establish whether the mass originates from the retroperitoneal soft tissue or a retroperitoneal organ. This distinction is clinically significant, as the composition of the lesion often helps in assessing whether it is likely to be malignant or benign (2).
We propose a structured approach to help radiologists refine the differential diagnosis:
Determine if the lesion is confined to the retroperitoneal space1. Tumor location : displacement of normal retroperitoneal organs, major vasculature, and their branches anteriorly strongly indicates that the lesion is situated within the retroperitoneum (4).
- Determine organ of origin:
- Beak or claw sign - When a mass forms an acute angle or a "beak"-like shape at the edge of an adjacent organ, it suggests an origin from that organ. In contrast, if the mass creates obtuse angles and smooth edges while compressing an organ, it is likely external to it (2).
 Fig 2: (A) Axial contrast-enhanced CT image reveals a mass that demonstrates a negative beak sign in relation to the right kidney. (B) Schematic diagram illustrating the negative beak sign. References : Iafrate, F., Ciolina, M., Venanzi, R., et al. (2016). Retroperitoneal tumors: A review of imaging features and differential diagnosis. Acta Radiologica, 57(5), 481–489
Fig 2: (A) Axial contrast-enhanced CT image reveals a mass that demonstrates a negative beak sign in relation to the right kidney. (B) Schematic diagram illustrating the negative beak sign. References : Iafrate, F., Ciolina, M., Venanzi, R., et al. (2016). Retroperitoneal tumors: A review of imaging features and differential diagnosis. Acta Radiologica, 57(5), 481–489 - Embedded organ sign- A mass lesion that does not originate from a hollow or malleable organ will deform it into a crescent shape, indicating a negative embedded organ sign. In contrast, masses arising from an organ tend to encase it, making the organ appear “embedded”
- Phatom organ sign - Large masses arising from small organs can obscure the native organ on imaging, rendering it “invisible.” (10)
 Fig 3: Axial contrast-enhanced CT image reveals absence of phantom sign which suggests primary retroperitoneal pathology. References :Kawashima, A., Sandler, C. M., Ernst, R. D., et al. (1999). Imaging of non-vascular retroperitoneal pathology. Radiographics, 19(1), 151–181.
Fig 3: Axial contrast-enhanced CT image reveals absence of phantom sign which suggests primary retroperitoneal pathology. References :Kawashima, A., Sandler, C. M., Ernst, R. D., et al. (1999). Imaging of non-vascular retroperitoneal pathology. Radiographics, 19(1), 151–181. - Prominent feeding artery- Hypervascular masses may have a prominent feeding vessel visible on CT, aiding in determining their origin.
Approaches for refining the differential diagnosis of primary retroperitoneal lesions
The following is a 3-step algorithmic approach to confirming the retroperitoneal origin of a mass and establishing an accurate diagnosis by systematically excluding differential possibilities .
First step : determine the lesion is retroperitoneal (displacing retroperitoneal organs) and to exclude organ of origin
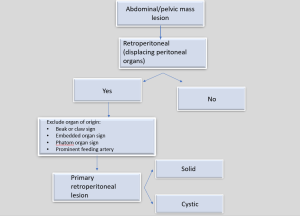
Second step: Based on the imaging appearance, classify the lesion broadly as solid or cystic
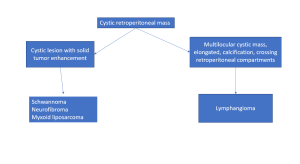
- it important to analyze all the components of a solid tumor to narrow the differential diagnosis
 Fig 16: A scheme for the differential diagnosis of solid retroperitoneal lesions according to composition
Fig 16: A scheme for the differential diagnosis of solid retroperitoneal lesions according to composition
Third step: Vascular and enhancement pattern of the lesion 
- There have been described 3 enhancement patterns
- Early enhancement with rapid wash-out- benign lesions
- Early enhancement with delayed wash-out – mostly malignant
- Delayed enhancement – myxoid or fibrotic components
Forth step: Location and pattern of spread and growth 
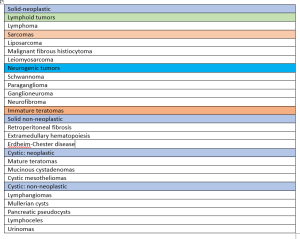
Solid primary retroperitoneal masses
Solid primary retroperitoneal masses can be broadly divided into neoplastic and non neoplastic categories