Congress:
ECR25
Poster Number:
C-25904
Type:
Poster: EPOS Radiologist (educational)
Authorblock:
R. A. Pugliesi1, G. Porrello2, K. Ben Mansour3, V. Rafailidis4, F. Vernuccio2, A. Papachristodoulou4, N. Maalouf5, J. C. Apitzsch5, R. Cannella2; 1Stuttgart/DE, 2Palermo/IT, 3Ludwigsburg/DE, 4Thessaloniki/GR, 5Pforzheim/DE
Disclosures:
Rosa Alba Pugliesi:
Nothing to disclose
Giorgia Porrello:
Nothing to disclose
Karim Ben Mansour:
Nothing to disclose
Vasileios Rafailidis:
Nothing to disclose
Federica Vernuccio:
Nothing to disclose
Angeliki Papachristodoulou:
Nothing to disclose
Nour Maalouf:
Nothing to disclose
Jonas Christoph Apitzsch:
Nothing to disclose
Roberto Cannella:
Nothing to disclose
Keywords:
Abdomen, Emergency, Paediatric, CT, Complications, Acute
This poster presents a case-based example series of pediatric trauma cases, highlighting key diagnostic pitfalls and practical strategies for improving accuracy in emergency settings (Table 2).
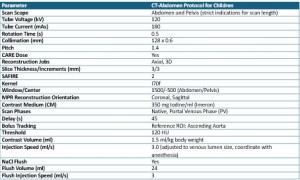
Table 2: Suggested CT-Abdomen protocol for the pediatric population (protocol used in Klinikum Ludwigsburg, Germany).
- Liver Trauma: A 15-year-old with several hepatic lacerations, adrenal hematoma, and pulmonary contusion illustrated the value of multi-phase CT for pediatric trauma imaging (Fig. 1). In the same manner, a 15-year-old patient with blunt trauma presented with B-mode ultrasound with hyperechoic liver laceration. Nonetheless, CEUS established the severity of the injury, illustrating the role of contrast-enhanced scans for indeterminate ultrasound findings (Fig. 2).
- Multisystem Trauma: A 17-year-old post-motor vehicle accident (MVA) with mediastinal widening and right-sided hydropneumothorax (Fig. 3) was confirmed by CT scans to have liver injury that needed angioembolization, demonstrating the role of optimized CT for rapid, artifact-minimized imaging. The example illustrates the need for high-resolution, contrast-enhanced imaging for children with possible polytrauma.
- Liver and Spleen Injury Grading: Trauma grading systems for liver and spleen injury (AAST Injury Scoring Scale) direct clinical management [3]. In children, imaging findings vary from superficial parenchymal trauma (Grade 1) to severe vascular injury (Grade 5) and require appropriate imaging protocol application to determine severity correctly [4,5]. A CT scan of a pediatric patient with Grade V splenic injury reveals >75% parenchymal disruption, active bleeding, and hemoperitoneum, highlighting the need for rapid, optimized CT (Fig. 4). Similarly, a 12-year-old with Grade V liver trauma exhibited extensive hepatic lobe disruption and retrohepatic vena cava involvement, emphasizing the critical role of contrast-enhanced imaging in severe cases (Fig. 5).
- Pelvic and Scrotal Trauma: A 15-year-old post-motorbike accident suffered a left scrotal rupture, iliac vein laceration, and significant pelvic hemorrhage (Fig. 6). Postoperative ultrasound confirmed vascular revascularization, emphasizing the utility of multimodal imaging approaches to pediatric pelvic trauma.
- Bowel Trauma: A 13-year-old with free fluid on post-traumatic ultrasound had collections of fluid but no bowel injury (Fig. 7). Small bowel injury was only established on follow-up CT, highlighting the failure of ultrasound alone in detecting hollow organ injury. Delayed-phase imaging remains very pertinent for the proper evaluation of bowel integrity in pediatric trauma.
- Renal and Pancreatic Trauma: A 17-year-old with a stab wound underwent CT revealing a renal laceration with perirenal hematoma (Fig. 8). CEUS demonstrated a non-enhancing laceration, but color Doppler was diagnostically unhelpful, again showing modality-specific renal trauma strengths and weaknesses. In another case, an 11-year-old presented with pancreatitis due to trauma with pancreatic swelling and fluid collections on ultrasound (Fig. 9). Imaging early is key to detecting pancreatic injuries that are otherwise occult on initial presentation.