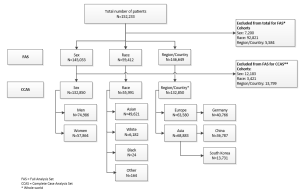
1.) The Phase-IV-Analysis comprised 152,233 patients from 37 countries. In the full analysis set 145,033 were included in the sex cohort, 59,412 in the race cohort and 146,649 in the region/country cohort.
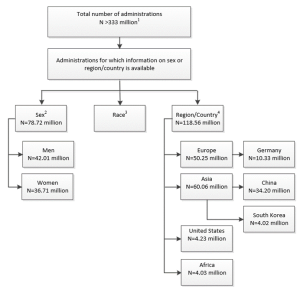
2.) The GPV-Analysis was based on 78.72 and 118.56 million administrations for which sex or region/country exposures were estimable.
Sex
1.) The Phase-IV-Analysis: The HSR incidence was significantly higher for women (0.72%) vs. men (0.55%) (p≤0.0001).

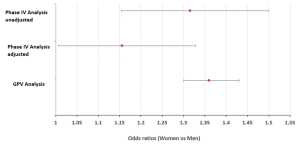
2.) The GPV-Analysis: Reporting rates were 0.0102% for women and 0.0075% for men (p<0.0001). The OR was 1.36 (CI 1.3, 1.43).
Race
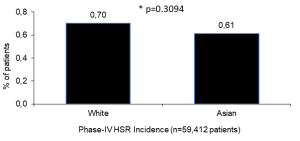
1.) In the Phase-IV-Analysis no significantly different HSR incidences for white (0.70%) and Asian (0.61%) patients (p=0.3094) were detected.
Region/country
1.) In the Phase-IV-Analysis the overall world HSR incidence was 0.62%. Europe: 0.52%, Asia: 0.70% USA: 0.75%, Germany: 0.51%, China: 0.41%, South Korea: 0.76%.
2.) In the GPV-Analysis the overall world HSR reporting rate was 0.015%, varying across regions/countries.

Limitations
- In Phase-IV-Analysis 7,200, 92,821 and 5,584 patients for sex, race, and region/country, respectively, had to be excluded upfront from FAS because of missing key data. In GPV-Analysis out of >333 million administrations only 78.72 million and 118.56 million were eligible for the sex and region/country evaluation, respectively. Race could not be analyzed at all as race is not captured by GPV and was not available in market research.
- Serious cases reported in the Phase-IV-Analysis of the 4 observational studies are necessarily also included in the GPV database. However, these were just 905 cases in 17,841 cases.
- In observational studies and even more in pharmacovigilance databases underreporting cannot be ruled out.