Lymphomas can arise in a variety of extranodal locations and exhibit diverse imaging characteristics that may complicate diagnosis. This review focuses on four notable atypical presentations: sinonasal lymphoma, renal lymphoma, cutaneous lymphoma, and central nervous system lymphoma. Each subtype demonstrates similar patterns in atypical locations, with minor variations due to adjacent tissue involvement.
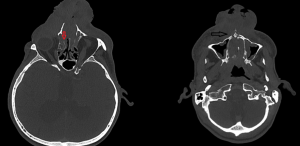
1. NK/T cell nasal lymphoma
The starting point is the mucosa-associated lymphoid tissue (MALT), which is already recognized as being particularly rich in this area. Multiple factors are involved in the pathogenesis of nasal lymphoma, including antigenic stimulation through chronic inflammation and also viral infectious agents such as Epstein-Barr virus, human T-cell leukemia virus type 1 (HTLV-1), and human herpesvirus-8 (HHV-8).
NK/T-cell nasal lymphoma is highly aggressive, with destructive lesions extending to the soft tissues and orbit, often with perineural spread, particularly involving the trigeminal nerve.
- CT appearance:
-soft tissue mass with ill-defined margins and heterogeneous, marked contrast enhancement, often causing septal perforation and extensive bone destruction, particularly in the maxilla and ethmoid.
- MRI appearance:
-T1-Weighted image: Iso- to hypointense relative to muscle.
-Contrast Enhancement (T1+C): Marked, heterogeneous enhancement with areas of necrosis.
-T2-Weighted image: Hyperintense but often heterogeneous due to necrosis.
-Diffusion-Weighted Imaging (DWI)/ Apparent Diffusion Coefficient (ADC): Restricted diffusion, indicating high cellularity.
- Nuclear medicine: Increased avidity on 18F-FDG PET-C

2. Cutaneous (scalp) lymphoma
Cutaneous lymphoma, particularly affecting the scalp, is a group of lymphoproliferative disorders in which malignant lymphocytes infiltrate the skin. It is classified into primary cutaneous lymphoma, which originates in the skin, and secondary lymphoma, which spreads from other organs. The pathophysiology involves the abnormal proliferation of T-cells or B-cells, leading to skin lesions.
Anaplastic large cell lymphoma (ALCL) comprises a group of T-cell lymphoproliferative disorders characterized by anaplastic cells that are CD30 positive and have variable expression of T-cell markers.
- CT findings :
-Well-defined or infiltrative soft tissue mass;-
-Mild to moderate enhancement with contrast;
-No significant bone destruction (unless advanced).
- MRI findings :
- T1-weighted image: Isointense or slightly hypointense to muscle.
- T2-weighted image: Hyperintense due to high cellularity and edema.
- Post-contrast T1: Heterogeneous enhancement, sometimes rim-like if necrosis is present.
- Diffusion-Weighted Imaging (DWI)/ Apparent Diffusion Coefficient (ADC): Restricted diffusion due to high cellularity.
- Nuclear medicine:
- Increased avidity on 18F-FDG PET-CT is almost always present.

3. Renal lymphoma
The kidney is an extranodal organ and does not contain lymphatic tissue. The precise etiology of this tumor has yet to be fully elucidated. Current hypotheses propose that PRL may originate from the renal capsule, subsequently infiltrating the parenchyma, or result from the infiltration of lymphoid cells into the kidney as a reactive process to chronic inflammatory conditions.
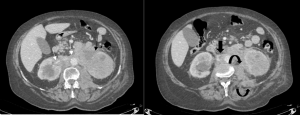
CT is the preferred imaging modality for the initial evaluation of suspected renal lymphoma due to its high sensitivity in detecting renal involvement, extrarenal spread, and involvement of other organs.
- CT findings:
- Lesion Characteristics:
- Renal involvement is often bilateral and may present as diffuse infiltration, or, less commonly, a solitary mass.
- Lesions are typically hypodense on non-contrast CT.
- Post-contrast imaging in the late arterial phase evaluates vascular structures and can distinguish lymphoma from hypervascular primary renal tumors. The nephrographic phase is essential for detecting smaller lesions.
- CT scans can identify necrosis, with non-enhancing hypodense areas on contrast-enhanced images indicating necrotic tissue within the tumor mass.
- Extrarenal Involvement:
- It may extend into the perirenal space, involve adjacent organs (liver, spleen), or appear in the psoas muscle. (Fig 5)
- Retroperitoneal lymphadenopathy is a hallmark of secondary renal lymphoma.
- MRI findings:
- T1-Weighted Imaging:
-
- Lesions appear hypointense compared to normal renal parenchyma.
- T2-Weighted Imaging:
-
- Lesions are mildly hyperintense.
- Post-Contrast (Gadolinium-Enhanced MRI):
-
- Lymphomatous deposits show mild, homogeneous enhancement similar to CT.
- Less enhancement compared to hypervascular renal tumors (e.g., renal cell carcinoma).

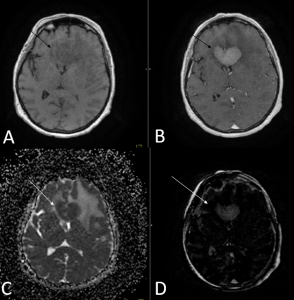
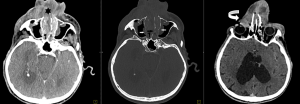
4. Central Nervous System Lymphoma (CNSL)
Central nervous system lymphoma is a rare extranodal lymphomatous malignancy that can affect the brain, spinal cord, leptomeninges, or vitreoretinal space. Most CNSLs are diffuse large B-cell lymphoma.
Patients with CNSL experience neurological symptoms that develop gradually over several weeks. These may include focal neurological deficits, neuropsychiatric changes, signs of increased intracranial pressure, and seizures. Clinical presentation is determined by neuroanatomical location of the lymphoma.
Radiologic evaluation is crucial to define the location and extension of the disease.
- CT appearance:
- Hypodense Lesions: On CT, CNS lymphoma often presents as hypodense masses, which may be homogeneous or slightly heterogeneous in appearance.
- Mass Effect: The tumors can cause a mass effect, including midline shift or compression of adjacent structures.
- Contrast Enhancement: The lesions usually show uniform enhancement after intravenous contrast administration, which helps distinguish them from other types of brain tumors like gliomas or metastases.
- Perilesional Edema: There may be surrounding vasogenic edema, which is common in CNS lymphoma.
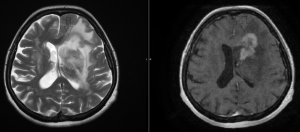
- MRI appearance:
- T1-weighted Images: hypointense compared to surrounding brain tissue.
- T2-weighted Images: hyperintense, indicating high water content, which is common in lymphomas.
- Contrast Enhancement: homogeneous or rim-enhancing contrast enhancement. It may appear as a solid, well-defined mass with surrounding edema.
-Periventricular Location: The tumor is often located periventricularly, in basal ganglia, or in the junction between the white and gray matter of cerebral hemispheres and less commonly in the brainstem.
-Infiltrative Growth Pattern: Lymphoma often shows an infiltrative growth pattern, which means it might not form a well-circumscribed mass and could spread into surrounding brain parenchyma.
The differential diagnosis is with high-grade gliomas; the key MRI distinction between central nervous system lymphoma (CNSL) and high-grade gliomas (HGG) lies in their enhancement pattern: CNSLs typically present with homogeneous enhancement, whereas HGGs often exhibit heterogeneous enhancement with areas of necrosis.