Updated Terminology for Defining Walls and Septa in Cystic Renal Masses
Determination of number of septa :
- Few : 1-3 septa
- Many : 4 or more septa

- BOSNIAK II : Thin(2mm) and few septa
- BOSNIAK IIF : Many thin septa
Determination of septa and wall thickness :
- Bosniak I: Smooth, thin, enhancing wall ≤ 2mm thickness, without septa.
- Bosniak II: Smooth, enhancing wall ≤ 2mm thickness, with 1-3 septa (each ≤ 2mm thick).
- Bosniak IIF: Smooth, minimally thickened wall or septa (3mm).
- Bosniak III: Any smoothly thickened wall or septa ≥ 4mm.

Distinguishing wall irregularity and nodularity :
Convex protrusions from a wall or septa can be categorized as nodules or irregular thickening. The distinction is made based on the angle formed with the wall / septum and its thickness.
Irregular thickening (Bosniak III feature) : Obtuse-angled enhancing areas are thickening if ≤ 3 mm.
Nodules (Bosniak IV feature) :
- Acute-angled enhancing areas are always nodules.
- Obtuse-angled areas are nodules if ≥ 4 mm (measured perpendicular to the surface).


When Not to Apply the Bosniak Classification :
The Bosniak classification is specifically designed for evaluating cystic renal masses and should not be used in the following scenarios:
- Lesions with Infectious, Inflammatory, or Vascular etiology :
- Cysts related to infection (e.g., abscesses), inflammation, or vascular abnormalities (e.g., aneurysms, AV malformations) do not fall within the scope of the Bosniak system.
2. Necrotic solid masses (>25% solid component) :
- Lesions where more than 25% of the mass consists of enhancing solid tissue are not true cystic masses but likely necrotic solid tumors. These typically exhibit more aggressive behavior than indolent cystic cancers and require different diagnostic considerations.
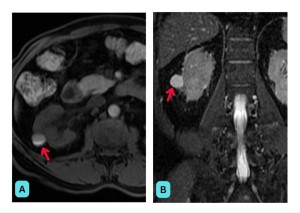
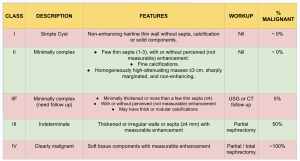
BOSNIAK Type I :
Bosniak I is considered a benign simple cyst. These cysts typically present as homogeneous, well-defined lesions with fluid attenuation values ranging from -9 to 20 Hounsfield units (HU). They are characterized by a thin, smooth wall measuring less than or equal to 2 mm in thickness, and they lack septations, enhancement, solid components, or calcifications.
The updated version allows wall enhancement after the administration of the contrast agent.
Bosniak I includes benign cysts, which do present no risk of malignancy, so they do need no follow-up.

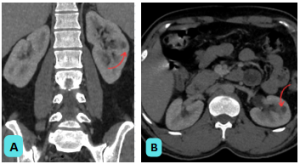
BOSNIAK Type II :
The Bosniak II classification encompasses benign renal cysts that are considered minimally complex. These cysts are typically well-defined and simple in appearance, but may exhibit one to three thin, hairline septa (≤2 mm in thickness) or fine calcifications. In some cases, perceived enhancement may be noted, and the cyst contents may be proteinaceous or hemorrhagic in nature.
Before categorizing a renal cyst as Bosniak II, it is essential to exclude any septal enhancement, as this could indicate a more complex lesion.
Six Types of Bosniak II Cystic Masses (All are well-defined with thin (≤2 mm) smooth walls) :
1. Cystic Masses with Thin Septa
- Thin (≤2 mm) walls and few (1–3) septa
- Septa and walls may enhance
- Possible calcifications of any type
2. Homogeneous Hyperattenuating Masses (≥70 HU) on Non-Contrast CT
- Appear uniformly hyperdense
- Typically benign, often proteinaceous or hemorrhagic cysts
3. Homogeneous Non-Enhancing Masses (>20 HU) on Renal Mass Protocol CT
- Higher attenuation but lack enhancement
- May contain calcifications
4. Homogeneous Low-Attenuation Masses (-9 to 20 HU) on Non-Contrast CT : Low attenuation, suggestive of simple cysts or fat-containing lesions
5. Homogeneous Masses (21 to 30 HU) on Portal Venous Phase CT : Intermediate attenuation, may require further evaluation
6. Homogeneous Low-Attenuation Masses Too Small to Characterize
- Small, subcentimeter cystic lesions
- Typically monitored rather than classified definitively
Like Bosniak I cysts, Bosniak II lesions are regarded as benign and are not associated with malignancy. Consequently, they do not require surveillance or surgical intervention.

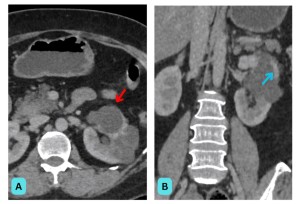
BOSNIAK Type IIF :
The Bosniak II F classification is applied to more complex renal cysts that are still generally well-defined but exhibit features that distinguish them from simpler cysts. These lesions may present with multiple (>4) thin septa (≤2 mm), and the calcifications present can be thick or nodular in nature. Both the walls and septa may appear smooth with minimal thickening (≤3 mm). While enhancement may be observed, it is typically not measurable. Additionally, this class may include intrarenal non-enhancing masses with high attenuation (>3 cm).
Bosniak IIF cysts have a 25% malignancy risk, requiring imaging surveillance every six months for a year, then annually. Monitoring duration varies from 1-2 years for less suspicious cysts to 3-4 years for higher-risk ones. Key concerns include morphological changes, solid component growth, and enhancement. Surgery is needed if progressive enhancement occurs.

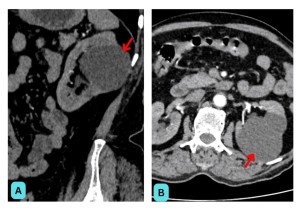
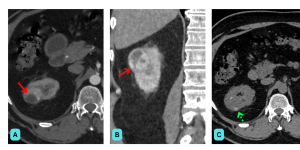
BOSNIAK Type III :
Bosniak III renal cysts are classified as indeterminate cystic masses that exhibit more complex features compared to the simpler classifications. These lesions typically present with irregular, smooth, or thickened (≥4 mm) walls or septa. The most crucial distinguishing characteristic of Bosniak III cysts is the presence of measurable enhancement. The updated classification now includes a defining feature where one or more walls or septa may display irregular enhancement, characterized by ≤3 mm obtusely margined convex protrusions.
Bosniak III cysts have a 50% malignancy risk, requiring surgery via partial or total nephrectomy or biopsy. Despite nearly half being benign, the high risk justifies surgical management over observation.

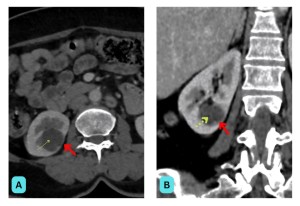
BOSNIAK Type IV :
Bosniak IV renal cysts are characterized as clearly malignant cystic masses, displaying all the features of Bosniak III cysts, with the addition of enhancing soft tissue components. These soft tissue components may be adjacent to or independent of the wall or septa. Bosniak IV lesions are specifically defined by the presence of one or more enhancing nodules, which may present as >4 mm convex protrusions with obtuse margins or any size convex protrusion with acute margins.
With a 90% malignancy rate, careful evaluation for local extension into adjacent structures (such as renal vein invasion) is essential. Given the high risk, urgent partial or total nephrectomy is necessary.
Knowledge Gaps in the Bosniak Classification, Version 2019
The 2019 update to the Bosniak classification improves malignancy prediction for cystic renal masses but leaves several important knowledge gaps unaddressed:
- Uncertain role of ultrasound (US) – While US can identify simple cysts, its role in classification is not fully established. Contrast-enhanced US may lead to higher Bosniak classifications than CT.
- Reliance on anatomic features – The classification is based on structural characteristics, while additional imaging parameters (e.g., perfusion, diffusion, chemical shift) might improve accuracy in predicting malignancy and aggressiveness.
- Unclear predictive value of individual features – The classification assumes certain features (e.g., septa thickness) correlate with malignancy, but the precise relationship and most predictive factors remain uncertain.
- Difficulty in differentiating cystic change from necrosis – Imaging struggles to distinguish benign cystic changes from necrotic RCCs, which may affect prognosis and treatment decisions.
- Mass size is not considered – Although smaller renal masses are more likely benign, size is not included in the classification. Growth patterns and morphology changes may be more relevant than absolute size.
- No assessment of tumor biologic behavior – The classification predicts malignancy but does not differentiate between aggressive and indolent cancers, leading to potential overtreatment. Further research is needed to refine surveillance and management strategies.