Anatomy
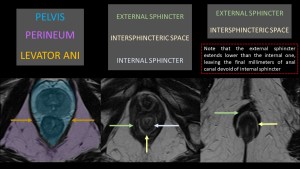
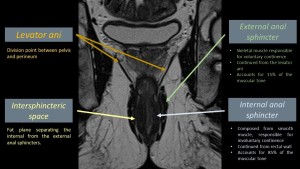
To talk about perianal fistulas, first must be discussed the anatomy of the anal canal and the perineum. The anal canal comprises the final 1 to 3 cm of GI tract and is the continuation of the rectum into the perineum. Anatomically, the pelvis and the perineum are separated by the levator ani muscle which will accompany the anal canal downwards comprising the external anal sphincter, while the internal anal sphincter is a continuation of the rectum wall. In between the sphincters, the intersphincteric space consists of a fat plane that separates both.
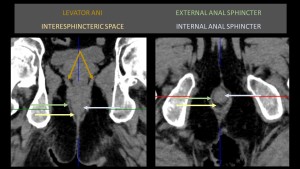
While the anal canal is usually studied via MRI, it is useful to be capable of recognizing the anatomy on CT scan for cases in which the sphincter must be studied in the emergency setting.
Imaging protocol
Perianal fistulas are studied with MRI for its better tissue definition, which can be lacking for this region on CT. The recommended protocol comprises of T1W, T2W, Fat-Sat and contrast-enhanced sequences.
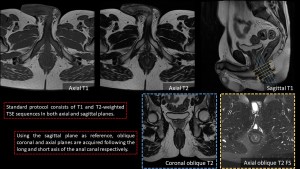
T1W axial and sagittal sequences are useful for an anatomical study and for the contrast-enhanced study, while T2W images are useful for detecting inflammatory changes.
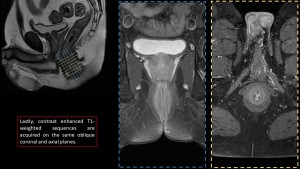
After axial and sagittal planes are acquired, the sagittal images are used for planning oblique coronal and axial planes, parallel and perpendicular respectively to the long axis of the anal canal.
Finally, T1W contrast-enhaced sequences are obtained in the oblique planes to assess contrast uptake.
Fistula assessment
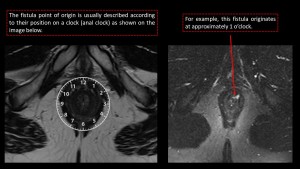
The first step in assessing a perianal fistula is locating its origin. The most common method for describing the origin of a fistula is the clock method, picturing the anal canal in an axial view as a clock and asigning an hour to the origin. This way fistulas originating at 3 o'clock would originate from the left-hand side margin of the anal canal, at 6 o'clock would be from the posterior margin, at 9 o'clock from the right-hand side margin and at 12 o'clock from the anterior margin.
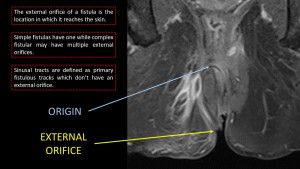
After the origin is located, the fistulous tract must be follwed to locate its external orifice, the point at which it breaches the skin. Depending on the complexity of the fistula it may have only one external orifice or it may have multiple, and on ocation a fistula origin can be seen with no external orifice, which recieves the name of sinusal tract.
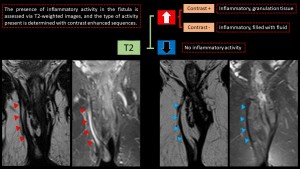
Finally, once the origin, the tract and the external orifice are located, fistulas must be assessed for activity. This is done with T2W and contrast-enhanced sequences. The presence of T2 hyperintensity indicates the existence of inflammatory activity, while contrast enhancement on T1 sequences denotes the presence of granulation tissue. Fistulas with low T2 signal and no contrast enhancement represent closed fistulas and scar tissue.
Classification
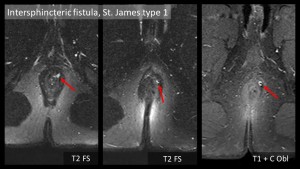
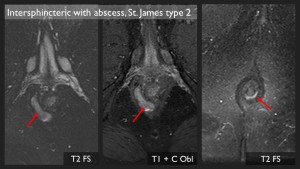
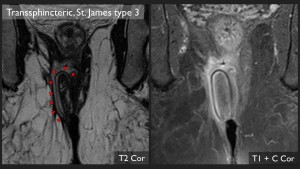
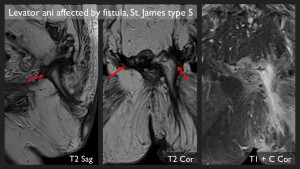
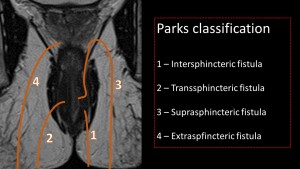
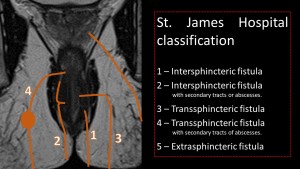
Two main classifications exist for the description of fistulas, the Parks classification and the St. James Hospital classification. Both are valid and preference for one or the other varies in each center, so good communication with the team of surgeons or specialists that will provide clinical manage for the patient will help in the creation of more efficient reports.
The Parks classification divides fistulas according to their main tract its direction and the anatomic structures involved, with secondary tracts and abscesses being described as complications of each class. On the other hand, the St. James Hospital classification takes into account secondary tracts and abscesses and they modify the grading of the fistula.
Examples