For a more dynamic review, we divided the findings according to the acronym TEACHES: 
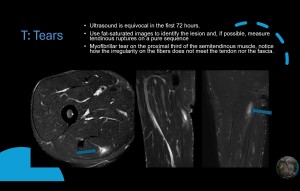
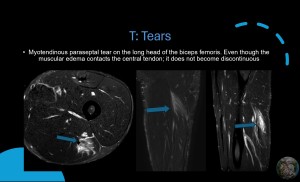
T: Tears
As described earlier, muscle tears must be evaluated according to the anatomical structures that were damaged. Tendinous and aponeurotic tissue involve longer recovery times. Also, ultrasound may not have the best findings in the first 72 hours. (2). Use fat-saturated images to identify the lesion and, if possible, measure tendinous ruptures on a pure sequence. Saturated images may exaggerate the length of the rupture.



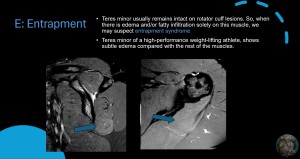
E: Entrapment.
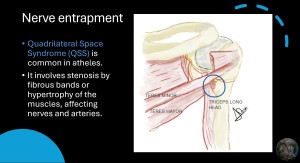
QSS is the most common entrapment on athletes, findings may be subtle but remember that the teres minor usually remains intact on rotator cuff lesions. So, when there is edema and/or fatty infiltration on this muscle, we may suspect entrapment syndrome.
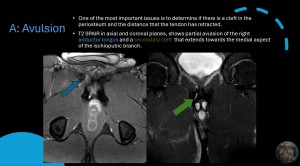
A: Avulsion.
When evaluating this type of lesion one of the most important issues is to determine if there is a cleft in the periosteum and the distance that the tendon has retracted. To assess the prior, oblique planes must be obtained following the direction of the affected bone.
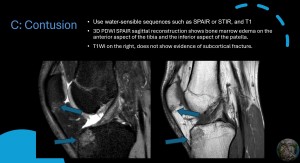
C: Contusion
Direct trauma may damage the trabeculae on the bone, as edema will gather around, water-sensible sequences such as SPAIR or STIR, and T1 will help us identify the findings. Also, on the T1W sequence, a linear hypointensity without disruption of the cortical bone may be indicative of a subcortical fracture.
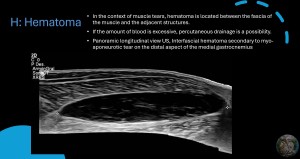
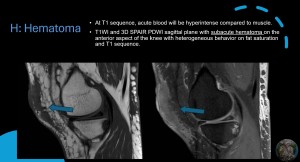
H: Hematoma
Hematic collections most likely have benign behavior. In the context of muscle tears, hematoma is located between the fascia of the muscle and the adjacent structures. On the leg, the interfacial space between the gastrocnemius, mostly medial, and soleus may be filled with blood during a myofascial or myotendinous rupture. Also, a rupture of the plantar tendon may be involved. If the amount of blood is excessive percutaneous drainage is a possibility. (13).
The importance of recognizing blood on MRI is that it imitates solid lesions, understanding that blood changes its behavior with elapsed time. A few tips are to evaluate the T1 sequence and compare it to the muscle since blood will be hyperintense compared to muscle. Also, in fat-saturated images acute blood may appear completely hyperintense, later it will begin to become heterogeneous and progressively hypointense.
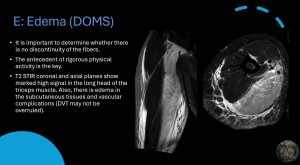
E: Edema (DOMS)
Notorious, but the important part is to determine whether there is no discontinuity of the fibers. The antecedent of rigorous activity is key.
S: Soft tissues.
Most findings on soft tissue have little connotation on the patient outcome, but one that should be evaluated and may at least require follow-up is the Morel-Lavallée lesions. Ultrasound is an adequate method for diagnosing, following up, and maybe treatment. (14).
