In our practice, athletes' most common extraarticular lesions are muscle and tendon tears. Ultrasound and MRI are the best choices for their evaluation. While MRI is the gold standard, recent studies show that ultrasound performed on a sports-centered facility is comparable(1).
Muscle fibers are disposed towards the central tendon. Tendons are inserted in the periosteum and cortex of the corresponding bone. Chains break on their weaker link, such as tears may appear where the fibers change their disposition or composition(2).
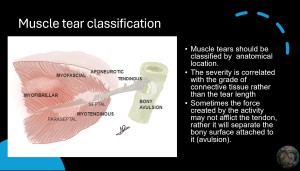
Muscle tears should be divided by their anatomical location. The gravity of the lesion is correlated to the grade of affection of the connective tissue rather than the length of the tear itself. In order of severity, the rupture may occur at the tendon insertion, aponeurosis, myotendinous junction, myofascial junction, and finally purely fibers rupture would be the least harmful(2,3).
Sometimes the force created by the activity may not afflict the tendon, rather it will separate the bony surface attached to it (avulsion). (4,5).
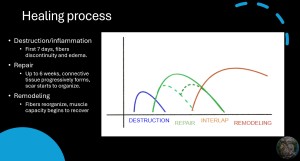
At follow-up, it is important to know the “normal” healing process. Until the 7th day of the injury the muscle fibers are surrounded by interstitial edema and the discontinuity of the tissue is present. Later, during the first 6 weeks, a scar of connective tissue progressively forms (repair), which can be divided into early and late stages. Later, the fibers start to reorganize during this process, and the muscle capacity will start to recover (remodeling). It must be said that these phases interlap, so when we look at control, we might find different evolution times. If the findings are too heterogeneous a re-tear might have occurred.

Edema is most likely indicative of acute injury in athletes, but sometimes it may not mean the muscle fibers are broken, as in delayed-onset muscle soreness (DOMS). (7,9) On the other hand, trauma may cause direct lesions on the bone structure, even without disruption of the cortical bone it will be seen as edema of the bone marrow. (4,5).
Sometimes, trauma may cause hematoma or edema on soft tissue, with the occasional presentation of the Morel-Lavallée lesions. Shearing forces are applied between the fat tissue and the underlying fascia potentially creating a space that may be filled with liquid collection (blood, lymph, fat necrosis, etc.). The treatment may be more complex than a common hematoma, especially when it becomes chronic. (10).
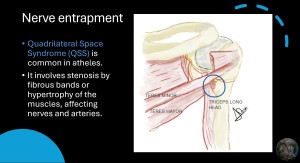
Other types of pain-inducing pathology are not trauma or stress-induced and are the entrapment of nerves. By far, the most common in athletes is the quadrilateral space syndrome (QSS)