[Look-alike ill-demarcated T2-low enlarged uterus]
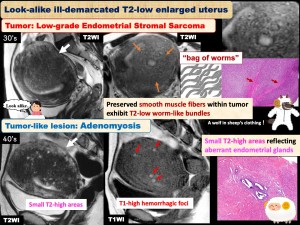
Tumor-like lesion: Adenomyosis
Tumor: Low-grade endometrial stromal sarcoma
[Adenomyosis]
- Common non-neoplastic disease characterized by the presence of ectopic endometrium within the myometrium
- Affects multiparous, premenopausal women with dysmenorrhea, menorrhagia, and abnormal genital bleeding
[Mimicker: Low-grade Endometrial Stromal Sarcoma: LG-ESS]
- Rare malignant mesenchymal tumor affecting young women
- May mimic adenomyosis, and characteristic myometrial invasion as “Bag of worms” (preserved T2-low smooth muscle bundles within T2-high tumor)
- Diffusion restriction (+)
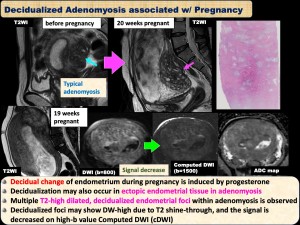
[Decidualized Adenomyosis]
- Decidualization during pregnancy may also occur in ectopic endometrial tissue in adenomyosis
- Multiple T2-high dilated, decidualized endometrial foci within adenomyosis is observed, which may mimic LG-ESS with “Bag of worms”
- Diffusion restriction (-), T2 shine-through (+)

[Look-alike localized ill-demarcated T2-low areas]
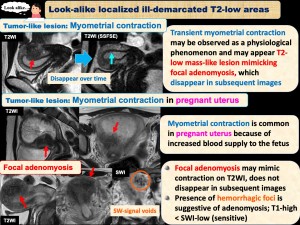
Tumor-like lesion (pseudotumoral lesion): Myometrial contraction
Tumor-like lesion: Focal adenomyosis
- Transient myometrial contraction may be observed as a physiological phenomenon and may appear T2-low mass-like lesion mimicking focal adenomyosis, which disappears in subsequent images. The appearance of lesions changes on kinematic MRI
- Myometrial contraction is common in pregnant uterus because of increased blood supply to the fetus
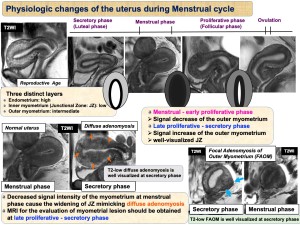
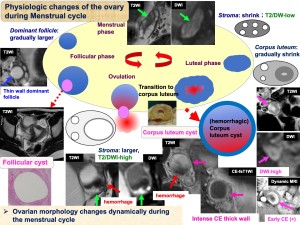
[Physiologic changes of the uterus during Menstrual cycle]
- The uterus undergoes significant changes depending on its physiological state and menstrual cycle, so a thorough understanding is essential for evaluating uterine lesions
[Look-alike ovarian cystic masses w/ hematocrit effect]
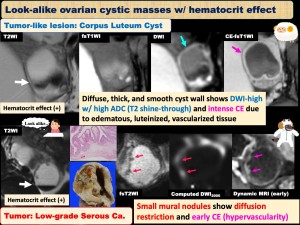
Tumor-like lesion: Corpus Luteum Cyst
Tumor: Low-grade Serous ca.
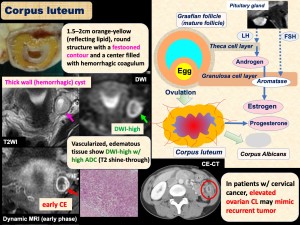
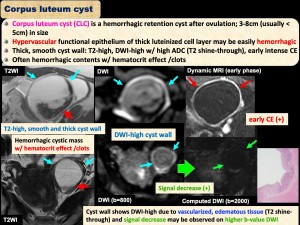
[Corpus Luteum / Corpus Luteum Cyst]
- Corpus luteum (CL) develops from an ovarian follicle during the luteal phase following ovulation
- Corpus luteum cyst (CLC) is a hemorrhagic retention cyst after ovulation. Hypervascular functional epithelium of thick luteinized cell layer may be easily hemorrhagic
- Smooth, thick wall w/ T2 shine-through vs Irregular, thick wall w/ diffusion restriction in cystic carcinoma
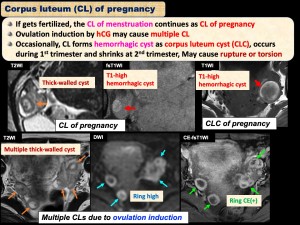
- If gets fertilized, the CL continues as CL of pregnancy and will release progesterone. Around week 12, the CL will start to break down
- Ovulation induction by hCG may cause multiple CL
- Occasionally, CL of pregnancy forms CLC, during 1st trimester and shrinks at 2nd trimester; May cause rupture or torsion
[Look-alike ovarian T2-low masses]
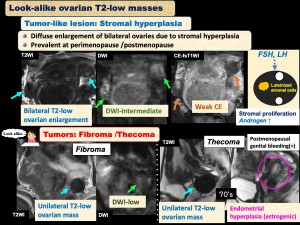
Tumor-like lesion: Stromal hyperplasia
Tumor: Fibroma /Thecoma
[Stromal hyperplasia]
- Diffuse enlargement of bilateral ovaries due to stromal hyperplasia (SH). Bilateral T2-low ovarian enlargement
- Prevalent at perimenopause /postmenopause
- Hyperthecosis (HT) is SH with luteinizing cell proliferation in response to increased gonadotropins; may be associated with masculinizing symptoms and menstrual abnormalities due to androgen production
[Look-alike ovarian masses w/ T2-peripheral low /central high]
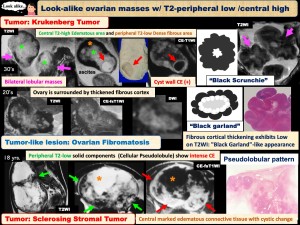
Tumor-like lesion: Fibromatosis
Tumor: Krukenberg tumor
Tumor: Sclerosing stromal tumor
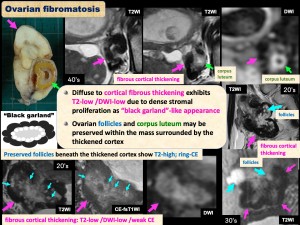
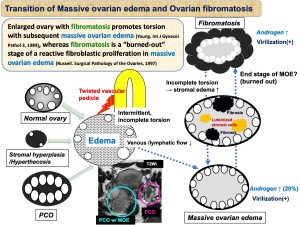
[Fibromatosis]
- Ovarian enlargement in young women affecting one or both ovaries
- Characterized by a proliferation of collagen-producing spindle cells surrounding normal ovarian structures
- Asymptomatic, or menstrual abnormalities, abdominal pain, hirsutism, or virilization
- Diffuse to cortical fibrous thickening exhibits T2-low due to dense stromal proliferation as “black garland”-like appearance. Ovarian follicles and corpus luteum may be preserved within the mass surrounded by the thickened cortex
[Look-alike T2-very high ovarian masses]
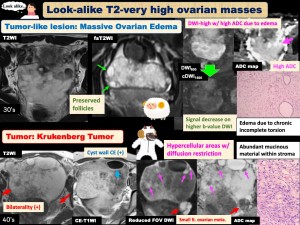
Tumor-like lesion: Massive Ovarian Edema
Tumor: Krukenberg tumor
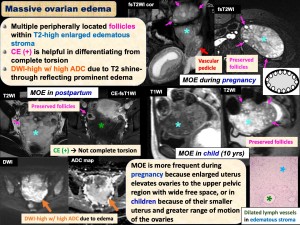
[Massive Ovarian Edema]
- Benign enlarged ovary affecting young women
- Intermittent torsion causes partial obstruction of venous /lymphatic drainage, accumulation of edema fluid within the stroma, and ovarian enlargement, T2-prominent high, T2 shine-through (+)
- Lower abdominal pain, intermittent of several months to years’ duration. Virilization in 20% of cases
- Diagnosis is important in selecting ovarian preservation treatment by laparoscopic untwisting or conservative management
[Transition of Massive ovarian edema and Ovarian fibromatosis]
- There is an argument: enlarged ovary with fibromatosis promotes torsion with subsequent massive ovarian edema, whereas fibromatosis is a “burned-out” stage of a reactive fibroblastic proliferation in massive ovarian edema
[Look-alike T2-high mural nodules in endometriotic cyst]
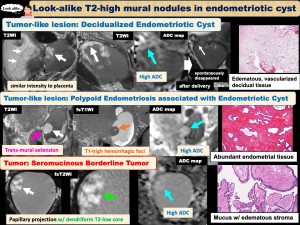
Tumor-like lesion: Decidualized Endometriotic Cyst
Tumor-like lesion: Polypoid Endometriosis
Tumor: Seromucinous Borderline Tumor
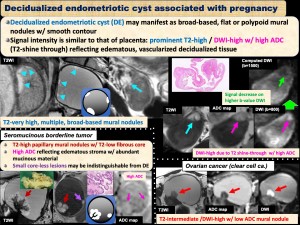
[Decidualized Endometriotic Cyst associated with pregnancy]
- Decidualized endometriotic cyst (DE) may manifest as broad-based, flat or polypoid mural nodules w/ smooth contour
- Signal is similar to placenta: prominent T2-high reflecting edematous, vascularized decidualized tissue. DWI-high w/ high ADC (T2 shine-through)
[Mimicker: Seromucinous Borderline Tumor: SMBT]
- Uncommon Müllerian-type tumor arising from endometriosis
- May affect relatively younger patients (30-40’s)
- Papillary mural nodules within endometrioma.
- Prominent T2-high reflecting edematous stroma w/ abundant mucinous material, T2 shine-through (+), mimicking DE
- The greater number and lower height are suggestive of DE, whereas lobulated margin, pedunculated configuration, and T2-low core (43-61%) of mural nodules are suggestive of SMBT
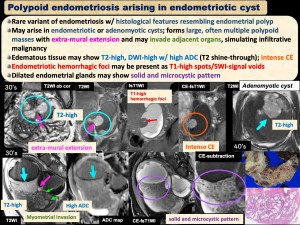
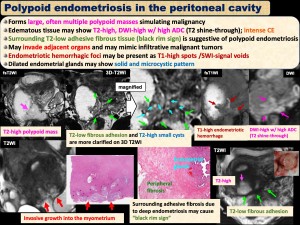
[Polypoid Endometriosis associated with Endometriotic cyst]
- Rare variant of endometriosis w/ histological features resembling endometrial polyp
- May arise in endometriotic or adenomyotic cysts; forms large, often multiple polypoid masses with extra-mural extension and may invade adjacent organs, simulating infiltrative malignancy
- Edematous tissue may show T2-high, intense CE, T2 shine-through (+), diffusion restriction (-)
- Endometriotic hemorrhagic foci may be present
- Dilated endometrial glands may show solid and microcystic pattern
[Look-alike bilateral ovarian multilocular cystic masses]
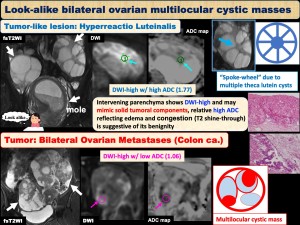
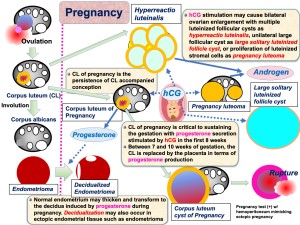
Tumor-like lesion: Hyperreactio Luteinalis
Tumor: Bilateral Ovarian Metastases (Colon ca.)
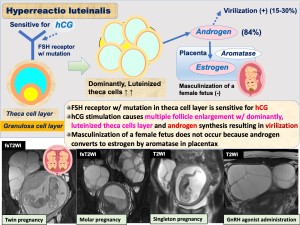
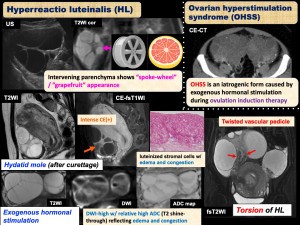
[Hyperreactio Luteinalis]
- Multiple theca lutein cysts caused by increased serum hCG, and hypersensitivity of FSH receptor w/ mutation
- Usually w/ gestational trophoblastic disease or polycyesis, rarely w/ normal pregnancy
- Regresses in size after delivery or removal of causative factors; Usually asymptomatic, occasionally cause torsion, intra-cystic hemorrhage, or rupture
- Marked bilateral ovarian enlargement w/ uniform multiple cysts separated by intervening parenchyma as characteristic “spoke-wheel” appearance
- Residual parenchyma may show T2-high, DWI-high w/ high ADC (T2 shine-through) vs multilocular malignancy w/ diffusion restriction
[Look-alike large ovarian cyst during pregnancy]
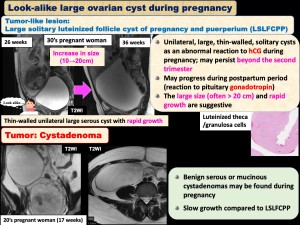
Tumor-like lesion: Large solitary luteinized follicle cyst
Tumor: Cystadenoma
[Large solitary luteinized follicle cyst of pregnancy and puerperium (LSLFCPP)]
- Unilateral, large, thin-walled, solitary cysts as an abnormal reaction to hCG during pregnancy; may persist beyond the second trimester (whereas functional cysts may spontaneously regress), mimicking cystic neoplasms
- May progress during postpartum period (reaction to pituitary gonadotropin)
- The large size (often > 20 cm) and rapid growth are suggestive
Pregnancy-related tumor-like lesions
[Look-alike cystic masses w/ mural nodule]
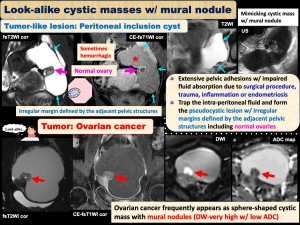
Tumor-like lesion: Peritoneal inclusion cyst
Tumor: Ovarian cancer
[Peritoneal inclusion cyst]
- Extensive pelvic adhesions w/ impaired fluid absorption due to surgical procedure, trauma, inflammation or endometriosis
- Trap the intra-peritoneal fluid and form the pseudocystic lesion w/ irregular margins defined by the adjacent pelvic structures, including normal ovaries
- Occasionally multiloculated and hemorrhagic, mimicking tumor; the ovary in the pseudocyst may simulate a solid tumoral component of cystic tumor
- May resolve spontaneously, and when asymptomatic, observation is initially chosen; therefore, differentiation from neoplastic lesions is crucial
[Look-alike Cul-de-Sac masses]
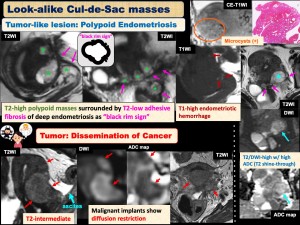
Tumor-like lesion: Polypoid Endometriosis
Tumor: Dissemination of Cancer
[Polypoid endometriosis in the peritoneal cavity]
- Forms large, often multiple polypoid masses simulating malignant implants
- May invade adjacent organs and may mimic infiltrative malignant tumors
- Edematous tissue may show T2-high, intense CE, T2 shine-through (+)
- Surrounding T2-low adhesive fibrous tissue (black rim sign) is suggestive of polypoid endometriosis
[Look-alike Bowel masses]

Tumor-like lesion: Bowel Endometriosis
Tumor: Bowel Cancer
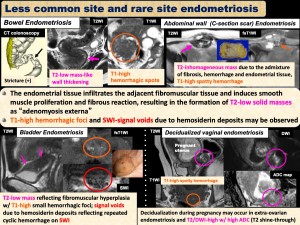
[Less common site and rare site endometriosis]
- The endometrial tissue infiltrates the adjacent fibromuscular tissue and induces smooth muscle proliferation and fibrous reaction, resulting in the formation of T2-low solid masses
- Hemorrhagic foci may be observed
- Diffusion restriction (-)
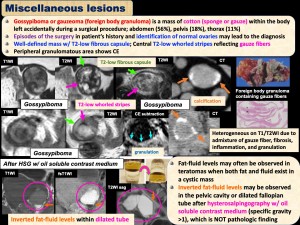
[Miscellaneous lesions]
[Gossypiboma or gauzeoma]
- Gossypiboma or gauzeoma (foreign body granuloma) is a mass of cotton (sponge or gauze) within the body left accidentally during a surgical procedure
- Well-defined mass w/ T2-low fibrous capsule; Central T2-low whorled stripes reflecting gauze fibers
- May mimic ovarian tumor, episodes of the surgery and identification of normal ovaries may also lead to the diagnosis
[After HSG w/ oil soluble contrast medium]
- Inverted fat-fluid levels may be observed in the pelvic cavity or dilated fallopian tube after hysterosalpingography w/ oil soluble contrast medium (specific gravity >1) for infertility screening
- May mimic fat-containing tumor (teratoma etc.), but NOT pathologic finding