1. To describe and illustrate the imaging spectrum of various hypervascular mediastinal masses.
2. To discuss in brief, the associated familial tumor syndromes and genetic mutations.
3. To highlight the importance of interventional radiological procedures in diagnosis and management.
4. To discuss potential pitfalls in making an accurate diagnosis on imaging.
The mediastinum is anatomically laterally demarcated by the pleural cavities, superiorly limited by the thoracic inlet, and inferiorly by the diaphragm.
It is often divided into convenient compartments.
In particular, mediastinum is compartmentalized into anterior, middle, and posterior divisions. A line extending from the diaphragm to the thoracic inlet along the back of the heart and anterior to the trachea separates the anterior and middle mediastinal compartments, whereas a line that connects points 1 cm behind the anterior margins of the vertebral bodies separates the middle and posterior mediastinal compartments.
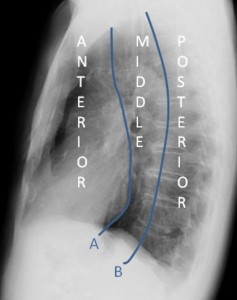
The anterior mediastinum contains thymus, fat, and lymph nodes, ascending aorta and heart. The middle mediastinum contains trachea, bronchi, aortic arch, brachiocephalic veins, esophageous, and lymphnodes, while the posterior mediastinum consists of the descending thoracic aorta, azygous vein, autonomic ganglia and nerves, thoracic lymphnodes, and fat.
The aim of this poster is to underline the imaging characteristics of hypervascular mediastinal masses and relatyed interventions. These lesions belong to a heterogeneous group with a broad age range. Among them, primary neuroendocrine tumors, vascular malformations, and lymphoproliferative disorders occur more often. Hypervascular lesions may also represent ectopic thyroid or parathyroid tissue. Rarely, do the enhanced masses represent hypervascular metastases or primary germ cell tumors.