
Normal swallow physiology
In order to identify abnormal swallow, one needs to recognise the normal phases of swallowing. Normal swallow physiology can be divided into 3 phases:
- Oral Phase
- Pharyngeal
- Oesophageal
The detailed components of each phase are shown below:




Common swallowing abnormalities can be classified based on which phase of swallowing they occur in.
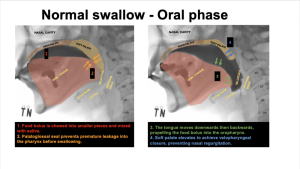
Oral phase
- Anterior loss
- Contrast is seen spilling out anteriorly from the mouth.
- Suggests weakness of orbicularis oris resulting in inadequate lip closure.
- Causes inclue: facial nerve palsy, myotonic dystrophy and myasthenia gravis.

- Sublingual loss
- Contrast is seen spilling below tongue.
- In preparation for swallowing, food bolus is usually held between the superior surface of the tongue and palate.
- Tongue weakness and loss of orolingual control results in poor control of the food bolus, resulting in sublingual loss.
- Premature spillage
- Contrast is seen spilling into the oropharynx before initiation of pharyngeal phase.
- Tongue and soft palate forms a seal (palatoglossal seal) posteriorly to prevent food bolus from moving into the pharynx before swallowing.
- Tongue weakness and loss of orolingual control can result in the inability to maintain the palatoglossal seal, resulting in premature spillage.

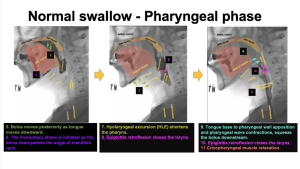
Pharyngeal phase
- Delayed onset
- Hyoid bone remains in resting position although contrast bolus has reached pharyngeal lumen.
- Increases the risk of penetration/aspiration due to an unprotected airway.
- Attributed to reduced pharyngeal sensory perception.
- Reduced base of tongue to posterior pharyngeal wall apposition (BoT-PPW)
- Seen as vallecular residue on the VFSS.
- The BoT-PPW apposition is the most important driving force of pharyngeal swallow which pushes the bolus down the digestive tract.
- If this is the primary abnormality, targeted therapy is viable (Masako manouevre).

- Reduced hyolaryngeal excursion
- Hyoid bone does not reach the inferior border of the mandible.
- Results in reduced epiglottic retroflexion and poor airway protection.
- Implies suprahyoid and pharyngeal elevator weakness. This can be further reduced in tracheostomy patients. Rehabilitation therapy can be performed (Shaker’s manouevre).

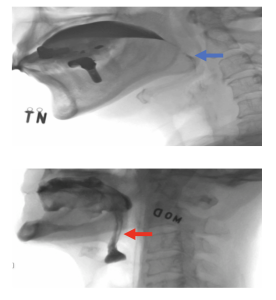
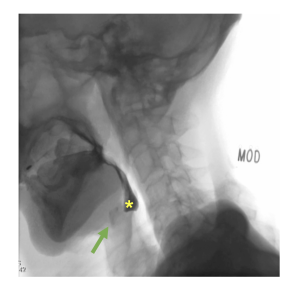
- Reduced/ delayed/ incomplete cricopharyngeus opening
- Results in pyriform sinus residue, which increases the risk of aspiration when respiration resumes.

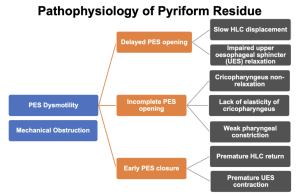
- Pyriform residue
- Can be caused by pharyngeal-oesophageal sphincter (PES) dysmotility or mechanical obstruction.
- The different pathophysiologies causing PES dysmotility is shown below:
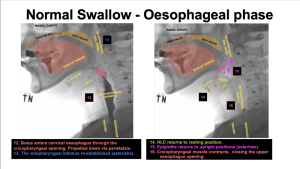
Oesophageal phase
- Oesophageal dysphagia is best evaluated with:
- VFSS – Subjective evaluation of oesophageal dysmotility
- Manometry – Objective evaluation of oesophageal dysmotility
- OGD – Rule out anatomical abnormalities
- VFSS provides a preliminary evaluation of oesophageal motility. Commonly seen oesophageal motility disorders on VFSS include:
- Delayed oesophageal transit
- Retrograde propulsion
- Gastro-oesophageal reflux
Oesophageal phase abnormalities can be classified into functional and structural causes.
Functional Abnormalities
- Delayed oesophageal transit - Subjective assessment of food bolus transit time through the oesophagus.
- The normal oesophageal transit is shown in Figure 17.
- Delayed transit can be a result of oesophageal hold-up of bolus (Figure 18) and retrograde propulsion.
- Cyclic ingestion can clear oesophageal hold up and improve transit time (Figure 19).



- Gastro-oesophageal reflux - Reflux precaution advice should be given to the patient.
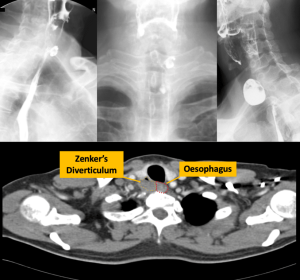
Structural Abnormalities
Dysphagia can be a result of structural abnormalities arising from anywhere between the oral cavity to the esophagus. Examples of these structural abnormalities include:
- Zenker’s diverticulum (Figure 20)
- Oesophageal diverticulum (Figure 21)
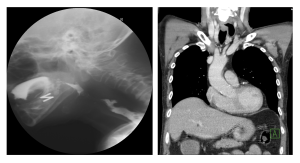
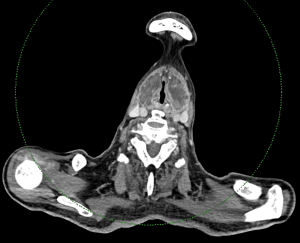
- Neck masses (Figure 22 and 23)

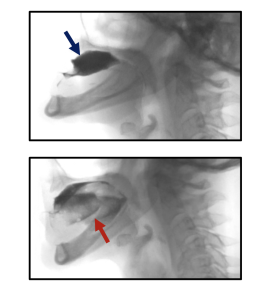
Penetration and Aspiration
- Penetration occurs when food/liquid/contrast enters the larynx, but remains above the vocal cords.
- Aspiration occurs when food/liquid/contrast passes below the vocal cords.
Teaching Point: Penetration and aspiration are the end result of the various swallowing pathophysiologies.
Case Examples
Most patients present with a combination of swallowing pathologies across different phases of swallowing. It may be difficult to identify these pathologies as the process of swallowing occurs rapidly in real-time. Although identifying these pathologies in real-time can be done by experienced clinicians, it is helpful to review the study in slow motion in order to ensure that subtle abnormalities are not missed. This is important in order to guide subsequent individualised rehabilitative therapy.
As such, 3 annotated case examples are provided below in slow motion to guide the interpretation of a VFSS.


