Internal hernias represent a complex pathological entity with a subtle and often confusing clinical presentation, making radiologist’s role crucial in accurate patient assessment. As with many acute abdomen cases, ultrasound (US) and conventional radiography are typically the first-line imaging techniques, especially in the emergency setting, with CT often being considered only at a later stage of the diagnostic process.
Conventional radiology and/or US may show unspecific signs of small bowel obstruction, such as dilated bowel loops with enlarged walls and intraperitoneal fluid resulting from the possible ischemic lesion associated with the bowel herniation and strangulation.
CT scan certainly shows more specific findings such as enlarged dilated bowel loops with a sac-like appearance, with signs of ischemia such as lack of mural enhancement, pneumatosis, interloop fluid, and abnormal bowel wall thickness. Another typical sign of IH on CT is the swirl sign characterised by the twisting and stretched appearance of mesenteric vessels towards the site of herniation.
A series of clinical cases is presented to showcase the diverse imaging appearance of internal hernias ranging from incidental findings to acute surgical emergencies. These patients were evaluated at the emergency radiology department of Ospedale Maggiore di Bologna where they initially underwent US and/or conventional radiographic examinations followed by contrast-enhanced CT studies.
CASE 1.
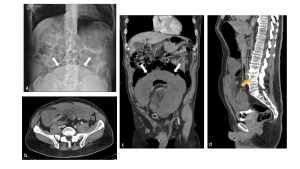
67 years old, male patient, presenting to the emergency department with acute abdominal pain and spontaneous loss of urine with history of renal and vesical litiasis. Patient firstly underwent conventional abdominal x-ray (fig 8.a) demonstrating diffuse bowel dilatation with no specific gas pattern, and a round opacity in the low quadrants suspected as bladder outlet obstruction. Contrast enhanced CT (fig 8.b,c,d) found a clustered sac-like appearance of dilated bowel loops in the low abdominal quadrants with stretched and engorged mesenteric vessels towards the site of the bowel cluster suggesting an Internal Abdominal hernia.
CASE 2
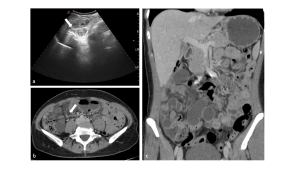
43 years old woman with abdominal pain prevailing in the right flank. The abdominal US exam (Fig 9.a) shows fluid filled dilated bowel loops in the right flank with associated peritoneal effusion in the right parietocolic shower. CT scan (fig 9.b-c) reveals at the site of the ecographic findings, a small herniation port with engorged and stretched mesenteric vessels with dilated fluid-filled bowel loops adjacent to the latter, suggesting a small bowel occlusion (SBO) due to internal hernia.
CASE 3

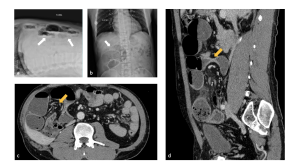
Male patient, 46 years old, admitted to the emergency department with persisting headache and epigastric pain arising in the morning accompanied by nausea. In his medical history he reports a previous appendectomy. First an abdominal ultrasound was performed (fig. 10.b) which showed the presence of some dilated fluid-filled bowel loops in the left side with an associated minimal fluid effusion between them. An x-ray of the abdomen (fig 10.a) is then performed, which confirms the presence of a few small bowel loops with different fluid levels in the middle abdomen and left flank in the absence of free air. On CT examination (10.c-d) distressed loops with vascular engorgement are revealed, with an associated stretched vascular pedicle conforming the classic “whirl sign”, highly suggestive of an internal hernia.
CASE 4
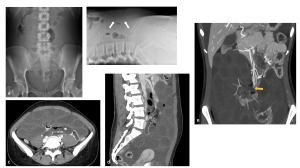
A 48-year-old male patient presenting with abdominal pain and constipation, with previous right kidney transplant surgery. On X-ray examination of the abdomen (11.a-11.b) some dilated small bowel loops in the right hypochondrium with associated air-fluid levels are appreciated. The CT scan (11.c-11.d) confirms the presence of packed multiple loops of the small intestine in the right lower-middle abdominal quadrants with stretched appearance of the mesenteric vessels. Additionally there is a C-shaped calibre transition point suggestive of closed loop bowel occlusion caused by internal hernia.
CASE 5
A 28-year-old female patient presents to the emergency department with diffuse abdominal pain. An initial abdominal X-ray in two projections (AP and tangential) (fig 12 a-b) shows a parietal thickening of some intestinal loops, likely of the small intestine, in the anterior abdominal regions. Subsequently, an abdominal CT scan with contrast (Fig. 12c–d-e) is performed, revealing a significant and widespread abdominal effusion with multiple dilated intestinal loops filled with fluid. The dilated loops also show signs of ischemic distress (parietal thickening and lack of contrast enhancement) associated with a stretched appearance of the mesenteric pedicle. The findings are highly suggestive of small bowel obstruction due to internal hernia with signs of advanced intestinal ischemia, requiring urgent surgical evaluation.
CASE 6
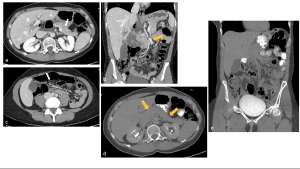
A 51-year-old woman presented to the emergency department with acute abdominal pain. An initial contrast-enhanced CT scan (Fig. 13 a-b-c) revealed a dilated small bowel loop in the mid-abdomen, near the liver hilum, displacing the pancreas laterally. The mesenteric vessels were also displaced laterally by the dilated loops and appeared stretched, with an associated twisting observed in the caudal slices.
The patient was then given an oral contrast solution, and a follow-up scan was performed (Fig. 13 d-e), showing resolution of the previous CT findings and re-establishment of normal anatomy, correlating with the patient’s clinical improvement. Further image evaluation confirmed the presence of a right paraduodenal internal hernia, which had spontaneously resolved after oral contrast administration.