There is a broad spectrum of pleura abnormalities, and ranges from: infections, systemic diseases, tumors or traumatic etiologies. [2]
Those pathologies can manifest as a pleural effusion, pneumothorax, pleural thickening and pleural calcifications.[3]
- Pleural effusions, the normal volume of fluid in each pleural space is aproximately 8 ml.[1] Pleural fluid are classified based on their compositions: exudates ex: empyema that can complicate with a bronchopleural fistula; or transudates ex: cirrhosis. Other specific causes of pleural effusion are chylothorax and hemothorax.
- Parapneumonic effusions and empyema
- Approximately 40% of patients with pneumonia develop an associated parapneumonic effusion, but only 10 % develop an empyema. Pneumonia is the most common cause of empyema. Contrast- enhanced CT is vital adjunct to pleural fluid analysis in managing patients with infected effusions or empyema in differentiating empyema from lung parenchymal abcess abutting the pleura. Is important to differentiation because attempted to dranaige a parenchymal abcess may seed the sterile pleural space with bacteria, whereas drainage is the therapy for empyema. Ultrasound is more sensitve that CT in detecting septations.[1]
- Pleural thickening may manifest as diffuse, focal/multifocal or unilateral/bilateral. Several normal findings can mimic the findings of pleural thickening or effusion, such as normal fat pads, subcostalis and transversus thoracic muscles and paravertebral intercostal veins.[3]
- Apical pleural Cap
- Apical opacities, or apical caps, are common nonspecific finding that my be idiopathic or seen in various disease states including infection, inflamatory, reaction to radiotherapy, neoplasm such as Pancoast tumor or peripheral upper lobe collapse.
- Usually are idiopathic asymtomatic irregular homogeneous densities less than 5 mm in tickness over lung apex. Commoly unilateral as bilateral, and are increasingly with aging ( over 45 years).
- When related to tuberculosis, tend to be thicker than idiopathic scars.
- Apical pleural caps may appear more irregular and are occasionaly difficult to distinguish from spiculated lung cancer. [1]
- Diffuse pleural thickening
 Fig 6: Portal phase CT- axial view Pleural Tuberculosis- Multifocal right pleural thickness. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 6: Portal phase CT- axial view Pleural Tuberculosis- Multifocal right pleural thickness. Department of Radiology, Hospital Beatriz Ângelo, Portugal Fig 5: Non-enhancement CT-axial view IgG4 related disease- focal thickness of posterior right costal pleura. This patient was submitted to biopsy. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 5: Non-enhancement CT-axial view IgG4 related disease- focal thickness of posterior right costal pleura. This patient was submitted to biopsy. Department of Radiology, Hospital Beatriz Ângelo, Portugal- Tuberculous or bacterial empyema, hemothorax ( especially posttraumatic, abestos exposure, radiation therapy, and some medications are the most common causes.
- Presence of rib fractures and normal lung parenchyma may suggest pleural thickening due to prior hemothorax, whereas post-infectious may have volume loss or parenchymal scaring.[1,2]
- Pneumothorax is defined as gas within the pleural space, which may ou may not be under tension. Can be classified as spontaneous and can be associated with pulmonary diseases or traumatic. Predisposing conditions include emphysema, pulmonary fibrosis, cyctic fibrosis, cavitary pneumonia, and cystic interstitial lung diseases.[1]
- Tension pneumothorax is a life threatening condition, and together with clinical symptoms, chest radiography has a crucial role.[1]
- Pleural calcifications may be seen in numerous conditions, including asbestos-related pleural disease, resolved hemothorax and pyogenic or mycobacterial infections.
Differential diagnosis of pleural masses
- Solitary fibrous tumor of the pleura
 Fig 7: Portal phase CT- axial view Left benign pleural solitary fibrous tumor. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 7: Portal phase CT- axial view Left benign pleural solitary fibrous tumor. Department of Radiology, Hospital Beatriz Ângelo, Portugal Fig 8: Portal phase CT- axial view Right malignant pleural solitary fibrous tumor. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 8: Portal phase CT- axial view Right malignant pleural solitary fibrous tumor. Department of Radiology, Hospital Beatriz Ângelo, Portugal- Rare mesenchymal fibrous origin that may be benign (80%) ou malignant (20%).
- The imaging apperance depends on size.
- Large lesions may have areas of myxoid change, hemorrhage, necrosis or cystic degeneration, and may contain calcifications. [1,2]
- Lipoma[1];[2]
 Fig 4: Non-enhancement CT-axial view Right pleura lipoma. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 4: Non-enhancement CT-axial view Right pleura lipoma. Department of Radiology, Hospital Beatriz Ângelo, Portugal- Rare in the pleura and show characteristics of fat in all imaging modalities.
- Well circumscribe, fat attenuation lesion on CT and MR they are hyperintense on T1 and moderately intense on T2-weighted images, with suppression on fat-saturated sequences and chemical shift artifact at their interfaces with fluid-rich tissues.
- Maligant pleural mesothelioma[1]
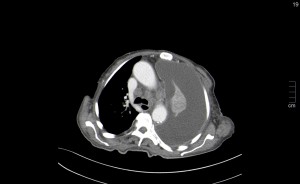
 Fig 3: Portal phase CT- axial view Mesothelioma- Irregular thickening of right costal and mediastinal pleura. Right pleural effusion. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 3: Portal phase CT- axial view Mesothelioma- Irregular thickening of right costal and mediastinal pleura. Right pleural effusion. Department of Radiology, Hospital Beatriz Ângelo, Portugal- Agressive tumor arising from the parietal pleural surface, most likely due to expossure do abestos.
- The most common clinical presentation is an elderly male with pleural effusion and pleuritic chest pain who has history of exposure to asbestos.
- Focal mass and advacend disease difficult to distinguish from advanced lung cancer.[2]
- Pleural metastases
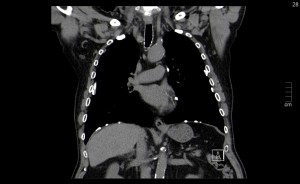
 Fig 2: Portal phase CT-coronal view Adolescent with osteosarcoma of femur, with pleural metastasis. Department of Radiology, Hospital Beatriz Ângelo, Portugal
Fig 2: Portal phase CT-coronal view Adolescent with osteosarcoma of femur, with pleural metastasis. Department of Radiology, Hospital Beatriz Ângelo, Portugal - Primary pleural sarcoma
- Rare tumors, and include liposarcoma, synovial sarcoma and undifferentiated pleomorphic sarcoma.[1]
- Epithelioid hemangioendothelioma [1]
There are other rare conditions such as thoracic splenosis, that is usually an incidental finding.
