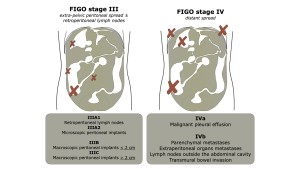
CT is the modality of choice for staging ovarian cancer and serves as an imaging substitute for the International Federation of Gynecology and Obstetrics (FIGO) classification system (Fig. 1). [1]
Scans of the chest, abdomen, and pelvis should be performed, usually done with both oral and intravenous contrast materials, except in cases where they are contraindicated. The use of positive oral contrast aids in visualizing bowel loops and identifying peritoneal deposits, particularly those involving the serosa and mesentery. Although, small calcified implants, more commonly associated with low-grade serous tumors, might be obscured by positive oral contrast, so in such instances, negative oral contrast materials are more effective for identifying these implants. [2]

Most of the patients (up to 70%) present with an advanced disease at the time of presentation [3] corresponding with FIGO stage III and stage IV (Fig. 2), so a complete macroscopic resection is the goal, dramatically affecting the disease-free survival and the overall survival rates [4, 5].
Complete macroscopic resection (R0) or eventually suboptimal resection (R1 = residual disease < 1 cm) is the desired result with primary debulking surgery (PDS). Therefore, CT staging serves as a tool to evaluate its feasibility compared to neoadjuvant chemotherapy with interval debulking surgery (IDS).
The criteria of resectability are not uniform and differ at each center and according to the actual experience of the surgical gynaecologist. Universally, the patient has to be fit to undergo the surgery and must benefit from it.
The role of us, radiologists, is to report the potentially unresectable disease as well as monitor the ongoing treatment response.
ROUTE OF PERITONEAL SPREAD
Peritoneal fluid preferentially circulates in a certain direction and is anatomically limited to certain areas. It flows in both directions and is pulled by gravity back to the pelvis.
All peritoneal recesses communicate with each other, however, peritoneal fluid from the pelvis primarily rises through the right paracolic gutter and forms the continuity of the inframesocolic and supramesocolic recesses on the right. On the left, the phrenicocolic ligament limits the left paracolic gutter from the inframesocolic recess.
From the right paracolic space, fluid continues into the right subhepatic space (Morrison's pouch) and can enter the omental bursa at the foramen of Winslow between the portal vein and the inferior vena cava. Fluid continues to the right subphrenic space due to lower pressure gradient here, but the falciform ligament usually limits right-to-left flow.
Therefore, peritoneal metastases with ovarian cancer are most frequent in the right paracolic, subhepatic and subphrenic spaces. Right diaphragm metastases are quite common and are one of the most overlooked.
Although falciform and phrenicocolic ligaments typically limit peritoneal fluid flow, they can be overflowed, for example with large amounts of ascites (mechanically, under the free edge of the falciform ligament and over the phrenicocolic ligament) [6].

MENTION THESE
The high-yield lesions that are critical to report are those that hold significant importance for surgical planning, particularly lesions that are potentially unresectable. Emphasis should be placed on identifying and documenting these lesions, as they directly impact the feasibility of surgical intervention and the choice of surgical approach.
RIGHT UPPER QUADRANT
- liver capsule implants with parenchymal invasion
- lesser sac implants
- porta hepatis implants or lymphadenopathy
- solitary or limited hepatic disease
LEFT UPPER QUADRANT
- gastrocolic ligament
- bursa omentalis implants
- lesser omentum implants
- solitary or limited gastric disease
CENTRAL AXIS
- peripheral or limited mesentery disease
- suprarenal retroperitoneal lymphadenopathy
PELVIS
- vascular encasement
- ureter invasion
- pelvic floor or abdominal wall invasion
HOW TO REPORT
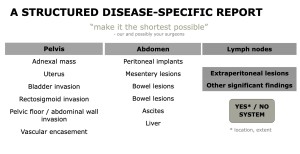
A structured, disease-specific report (Fig. 4) can greatly enhance clarity, as it provides a systematic framework to detail all key findings in a clean and easy-to-understand manner. This approach facilitates comprehensive communication between radiologists and surgeons. [7]
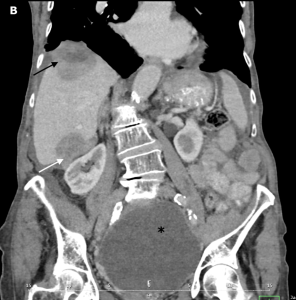
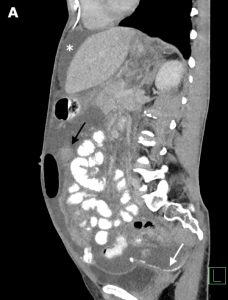
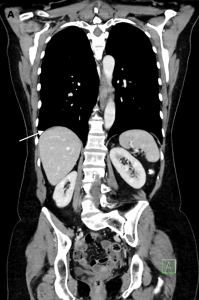
Examples of metastatic ovarian cancer from our clinical practice