General findings
Bony overgrowths on the lower limbs
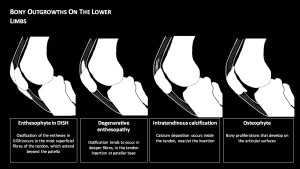
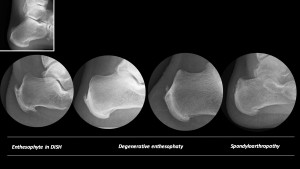
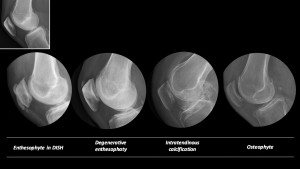
- DISH enthesophyte. The new bone shows characteristic solid well defined cortical margins without features of inflammatory change. This ossification occurs in the most superficial fibres of the tendon, which extend beyond the patella, and grows proximal and distally with a firm central attachment at the center of the anterior cortex of the patella
- Degenerative/overuse enthesopathy: calcification/ossification tends to occur in deeper fibres of the quadriceps entheses at patellar base.
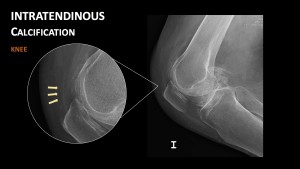
- Intratendinous calcification/ossification: calcium deposition occurs inside the tendon, near the insertion. This process occurs in CPPD, usually as linear deposit or discrete densities, and in tendon scarring processes.
- Osteophytes: formation of bone overgrowth at the margins of the articular cartilage (marginal osteophytes), originally as overgrowths of cartilage and subsequently undergo endochondral ossification typically at the superior and inferior aspect of the patella.
The differential diagnosis of enthesopathies can also include avulsions, fractures, ligament or tendon rupture, localized infection, contusions, muscle strains, and malignancy.
KNEE
DISH
- Prevalence varies between 67-88%.
- Most common are ossifications around the patella, quadricipital and patellar tendon. The tendon fibres that ossify are the most superficial. These fibres form a continuation over the patella, called the prepatellar continuation of the quadriceps, giving its ossification the appearance of “gull wings”.
- Ossification of the tibial tuberosity, bony insertion of the anterior cruciate ligament, proximal tibioperoneal joint and fabella may occur.

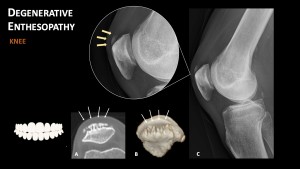
Degenerative/overuse enthesophaty
Overuse injuries of the extensor mechanism of the knee are common in both athletes and non-athletes and usually occur during activities associated with repetitive loading, stress, and knee extension.
Degenerative quadriceps tendon changes result in enthesophyte formation and vertical ridging at its superior patellar insertion site, giving rise to the "patellar tooth" sign. This sign is seen in the skyline (sunrise) view as saw-tooth projections.
Enthesopathy at the proximal insertion of the patellar tendon or "jumper's knee" is also typical, resulting from repeated forced extension. Inflammatory changes can be observed and may be accompanied by enthesophyte formation at the lower pole of the patella.
Intratendinous calcification
Osteophytes

FOOT
DISH
The most distinct features are calcaneal enthesophytes present at both the Achilles insertion and the plantar fascia, giving the calcaneus an "armoured" appearance.
Ossification of the insertion of the peroneus brevis muscle at the base of the fifth metatarsal and metatarsophalangeal para-articular ossifications can also be observed.

Degenerative enthesophaty
In the foot, the typical mechanical injury is enthesopathy of the plantar aponeurosis. Lateral radiography of the foot may show ossification of the calcaneal enthesis or "heel spur". In practice, the presence of a calcaneal spur on X-ray is very common and is not related to symptomatic calcaneal enthesopathy.
Insertional tendinopathy of the Achilles tendon occurs more frequently in the active population, being more frequent in runners, with an estimated prevalence in this group of between 6.5 - 18%.

Spondyloarthropaties
Enthesophytes are quite frequent in spondyloarthropathies. In patients with psoriasis, a calcaneal spur is present in up the 75% of the cases, and the Achilles tendon spur in 30% of them.
The presence of fluffy plantar periostitis and broad based and longer mid-segment dimensions are radiological features for inflammatory spurs.