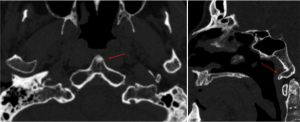
THIRD CONDYLE (prevalence: about 0.5%) (Prescher, Brors, and Adam 1996)
It forms when the median portion of the hypochordal arch persists. It is an anterior median bony process that originates from the anterior margin of the foramen magnum and may articulate with the odontoid process of the axis or with the anterior arch of the atlas. Sometimes it may be a free element, and in such cases, it should not be confused with the os terminale (which is associated with odontoid hypoplasia). Although usually asymptomatic, some studies have observed an association with C1-C2 instability (Saccheri and Travan, 2022; Figueiredo et al. 2008).
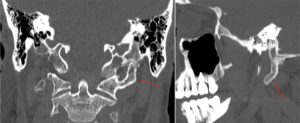
BASAL PROCESS (Prevalence 3-7.5%) (Figueiredo et al. 2008; Prescher, Brors, and Adam 1996)
It forms when the lateral portion of the hypochordal arch persists. It appears as a protuberance located antero-medially to the occipital condyles, along the anterior profile of the foramen magnum; it can be unilateral or bilateral, and sometimes two basal processes may be partially fused at the midline (false third condyle). The basal process is asymptomatic in most cases. Rarely, it may articulate with the anterior arch of the atlas or with the odontoid process of the axis (Saccheri and Travan, 2022).

PRE-BASIOCCIPITAL ARCH (prevalence: 0,03%) (Lombardi 1961)
It forms if the entire hypochordal bow of the proatlas persists and undergoes ossification, representing the combination of a third condyle and a basal process. It is a rather rare condition. In some cases, only partial regression occurs, so it is assimilated to the anterior profile of the foramen magnum. If regression does not occur at all, the "Napoleon's hat" sign may appear on coronal images (Prescher, Brors, and Adam 1996). It may be asymptomatic or cause pain during neck movements (Prescher, Brors, and Adam 1996; Saccheri and Travan 2022).

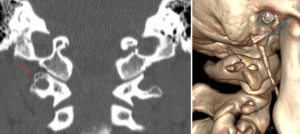
PARACONDYLAR PROCESSES: (prevalence: 0.077-0.29%) (Nolet, 1999)
The paracondylar processes, sometimes erroneously called paramastoid processes, is a broad-based bony cone originating from the exo-occiput, next to the occipital condyle, and directed downward toward the transverse process of the atlas.
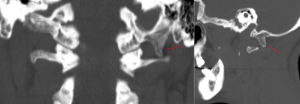

EPITRANSVERSE PROCESS:
The epitransverse process is a vestige of the cranial half of the first cervical sclerotome, forming a bony process originating from the transverse process of C1 and projecting upward toward the occipital bone. Epitransverse process can sometimes form a false joint with the occipital bone or with coexisting paracondylar process and may be associated with restricted neck movement (Shapiro and Robinson 1976; Saccheri and Travan 2022).
PONTICULUS POSTICUS (CT prevalence: about 8%)
Also called Kimmerle anomaly or arcuate foramen, it represents a relatively common anomaly, especially in women. It originates from the uni- or bilateral, partial or complete ossification of the posterior atlanto-occipital membrane, appearing as a bony bridge extending from the posterior part of the superior articular facet to the posterior arch, where the distal part of the vertebral artery is located. The pathogenesis is debated between genetic and post-traumatic causes. It may be asymptomatic or, in some cases, associated with compression of the vertebral artery and C1 nerve root (Zhang et al. 2023; Gul and Atik 2024; Golpinar et al. 2022).
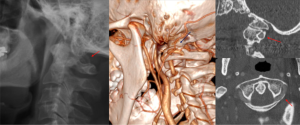
PONTICULUS LATERALIS (CT prevalence: about 4.67%)
The ponticulus lateralis is a bony bridge extending from the posterolateral part of the superior articular facet of the atlas to the transverse process, where the groove for the proximal part of the vertebral artery is normally found (Zhang et al. 2023).
As mentioned above, understanding these anatomical variants is important due to their potential clinical implications. The third condyle and basal processes, although often asymptomatic, may form false joints with the apex of the odontoid process of the axis or with the anterior arch of the atlas, which may undergo degenerative changes and become a source of pain. The paracondylar and epitransverse processes, especially when particularly pronounced, in addition to creating a mechanical obstacle to neck rotation, may also form false joints, with similar results. The ponticulus posticus, as noted, can cause compression of the vertebral artery and C1 nerve and an association has been found with migraines, vertigo, vertebrobasilar insufficiency, neck pain, and hearing loss. The presence of the ponticulus is also relevant in surgical procedures, as it may give the impression that the posterior arch of the atlas is wider than it is, increasing the risk of vertebral artery damage (Golpinar et al. 2022; Mokhtari et al. 2022; Najmuddin 2022).