The exploration of mandibular tumors begins primarily with panoramic radiography, followed by a CT scan or ConeBeam. For maxillary lesions, direct ConeBeam exploration is required.
In most cases, panoramic radiography (OPT) is sufficient for a positive diagnosis, but a CT scan allows for a more detailed characterization of radiolucent odontogenic tumors by defining their contours, densities, and extensions.
Odontogenic tumors exhibit a wide range of lesions and pose challenges in radiological diagnosis, as their radiographic features are often very similar, if not misleading. the occurrence of combined lesions is common. Hence, the importance of comparing with clinical data and histopathological results.
A. Odontogenic tumors:
I.Epithelial odontogenic tumors without mesenchymal induction:
- Ameloblastoma:
The ameloblastoma frequently presents as a slow-growing submucosal mass, loose teeth, malocclusion, paresthesias, and pain [2]. It has no gender predilection and peaks in incidence between the ages of 30 and 40. It corresponds to a proliferation of epithelial islands within a normal fibroconnective stroma. It presents in three forms: desmoplastic, plexiform, and unicystic, with dentigerous cyst being a differential diagnosis.
On the OPT, the lesion is often multilocular, multigeodic, creating the classic "soap bubble" appearance causing ballooning and thinning of bone cortex, with the frequent presence of an included tooth suggestive of the diagnosis. It is often associated with root resorption.

On a CT scan, tissue structures associated with cystic lesions may be observed, and these structures may enhance after contrast agent injection (although the use of contrast is optional). In some cases, cortical disappearance may be noted; it becomes significantly thinned and becomes undetectable on the CT scan, with cone-beam imaging being particularly effective for bone studies.

While classified as benign neoplasms, ameloblastomas exhibit a notable recurrence rate typically falling within the range of 5% to 30% over periods spanning from 5 to 15 years, thereby warranting the need for surgical resection [3]. They usually progress slowly, are locally invasive and, if left uncontrolled, may cause significant morbidity.
- Squamous odontogenic tumour (SOT):
Another benign odontogenic tumor in this category – that of neoplastic epithelium in the absence of odontogenic ectomesenchymally derived tissues – is the squamous odontogenic tumor. It is rare, benign, yet locally infiltrative epithelial tumor that is believed to originate from the remnants of dental lamina or gingival epithelium [4]. It presents as a radiotransparent lesion, either unilocular or multilocular, developing between the tooth roots.
- Calcifying epithelial odontogenic tumor (Pindborg’s tumor):
It is an extremely rare tumor, accounting for only 1% of odontogenic tumors [5].
The Pindborg tumor preferably occurs in the mandible, with an equal prevalence among men and women and a peak around the fourth decade of life. The clinical presentation is nonspecific.
On the radiological level, it is an expansive intraosseous odontogenic lesion, evolving slowly, initially radiolucent and well-defined. Its boundaries become more irregular as it increases in size, presenting a multilocular configuration. Calcifications are commonly observed, becoming indicative, and increase in size and number as the lesion evolves.
An included tooth or an odontoma is associated in 60% of cases. The polymorphic nature of the calcifying epithelial odontogenic tumor is reflected in its radiological appearance, which depends on the stage of maturation and the extent of the calcified component.

- Adenoid ameloblastoma
The adenomatoid odontogenic tumor is rare, accounting for 2 to 3% of odontogenic tumors. Approximately 40 cases have been reported in the literature so far [1]. The inclusion of Adenoid Ameloblastoma (AA) is the sole new addition in the odontogenic lesions category in the WHO 2022 classification, signifying the most significant change. It more commonly affects women and is usually located in the maxillary bone, especially in the incisor-canine region. Clinically, it manifests as a painless and gradually enlarging swelling or delay in tooth eruption. On panoramic radiography (OPT), the tumor appears as a well-defined radiolucent image, frequently accompanied by an impacted tooth. On CT, A radio-opaque component, resembling poorly mineralized dentin, is identified [3].
II.Benign mixed epithelial & mesenchymal odontogenic tumors:
Epithelial odontogenic tumors with ectomesenchymal induction constitute a seemingly heterogeneous group encompassing numerous initially complex tumors. These are tumors with a dual odontogenic epithelial and ectomesenchymal component. They exhibit tumor maturation following the stages of organogenesis seen in a normal tooth [3]. While rare, odontoma is the primary etiology within this group (20% of OT). Odontomas are regarded as hamartomas rather than neoplasms [6].
The odontoma is primarily located intraosseously, especially in the posterior mandible and anterior maxilla. Its discovery is often incidental, with a peak frequency between the ages of 20 and 30.
The odontoma presents in two forms: complex and compound.
- Complex: Aggregation of enamel and dentin mixed without morpho differentiation.
- Compound: Formation of the tooth with a small or malformed root and crown.
On imaging, it appears as a dental-tone opacity surrounded by a well-defined clear peripheral halo, situated within the body of the bone, and associated with the inclusion of one or more displaced teeth at the periphery.

III.Benign mesenchymal tumors:
Benign mesenchymal odontogenic tumors arise from the mesenchymal components of the tooth-forming apparatus, encompassing entities such as mesenchymal odontogenic fibroma, cementoblastoma, cemento-ossifying fibroma, and odontogenic myxoma being the most frequent [6].
Cemento-ossifying fibromas, slow-growing and usually painless, cause expansion. Displacement and pain are rare. Occurring mainly in the mandible's premolar and molar areas, they affect females in their second to fourth decades, with an average age of 35. Radiographically, they show a well-demarcated unilocular radiolucency with variable opacification based on hard tissue production.


B. Cysts of the jaw:
Regarding cystic lesions in the tooth region, the etiologies are dominated by 3 types of lesions: the radicular cyst, the dentigerous cyst, and the odontogenic cyst.
- Radicular cyst:
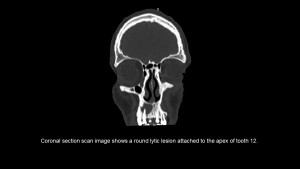
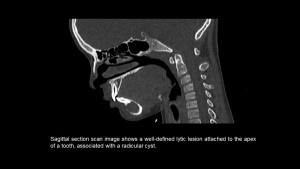
The radicular cyst is the most common cystic lesion of the maxillary sinuses (60%), representing the final stage of progression of the periapical inflammatory process. It follows the development of an apico-dental granuloma in contact with the decayed tooth, secondary to the necrosis of the pulp cavity. It is a well-defined lytic lesion adjacent to the apex of a necrotic or carious tooth.
- Dentigerous cyst:
The dentigerous cyst occurs more frequently in adolescents and young individuals. It manifests as a well-defined, round, purely lytic lesion developed around the crown of an impacted tooth, preferably located at the level of the mandibular third molar.
- Odontogenic keratocyst:
The odontogenic keratocysts are located in the maxillae and more frequently in the mandible, typically posteriorly in relation to the third molar and the ramus. In the maxilla, they are more commonly found at the level of the first premolar.
The lesion is often large (averaging 5 cm in length) and develops along the axis of the mandible [7].
