We will expose some cases from our institution according to body segments, explaining these signs and their interpretation.
Musculoskeletal system
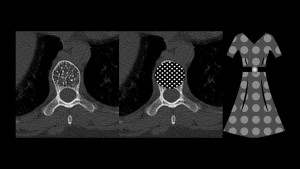
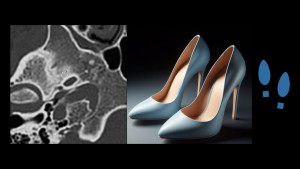
Polka dot: It consists of a pattern of small punctate areas of high attenuation seen in cross sectional CT studies, which represents trabecular thickening surrounded by fat marrow or vascular channels in vertebral hemangiomas.1
Scaphoid signet ring: It refers to the dense rounded cortex of the scaphoid tubercle on a posteroanterior radiograph due to subluxation from flexion of the scaphoid, that is seen in injuries of the scapholunate ligament or perilunate/lunate dislocations.2

Corduroy: This sign mimics the appearance of corduroy clothing and describes the appearance of thickened vertically oriented trabeculae seen in vertebral hemangiomas on lateral radiographs or sagittal CT scans.3


Rugger jersey spine: It refers to high attenuation densities endplates at multiple contiguous vertebral levels producing alternating sclerotic-lucent parallel bands that simulates the stripes on a rugby jersey. It’s distinctive for secondary hyperparathyroidism.3

Bow tie (discoid meniscus): It describes the body of a normal meniscus in continuity with the anterior and posterior horns on sagittal MRI of the knee. A discoid meniscus can be suggested on MRI when three or more bow tie shapes are identified on contiguous sagittal images (4-mm-thick). An absent bow tie sign is also suggestive of a bucket-handle tear.5

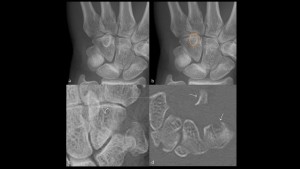
Ring sign (hook of the hamate fracture): On posteroanterior radiographs of the wrist the hook of the hamate normally overlaps with the midportion of hamate body and projects as an ovoid density. Signs of fracture of hook of the hamate include absence, discontinuity, displacement or sclerosis of the hook.6
Boutonnière deformity: It refers to pathologic flexion of the proximal interphalangeal joint (PIP) and hyperextension of the distal interphalangeal joint (DIP) of a finger. A disruption of the central aspect of the extensor tendon causes PIP flexion passing between the lateral bands, just as a button passes through a buttonhole. It is seen in inflammatory arthritis and traumatic tendon tears.7
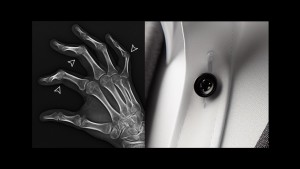
Button sequestrum: it consists of a bone opacity surrounded by a well-defined lucent area, resembling a button. It commonly represents eosinophilic granuloma or osteomyelitis.8

Neurological system
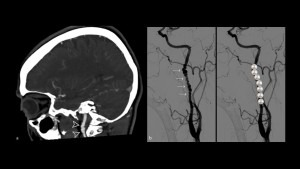
Stiletto footprint: It’s a useful sign to understand the skull base anatomy. The anterior aspect represents foramen ovale and the heel the foramen spinosum.9
String of pearls (fibromuscular dysplasia): It refers to the appearance of alternating dilation and multifocal stenoses in fibromuscular dysplasia.10
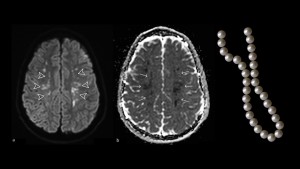
String of pearls (watershed cerebral infarction): It refers to the pattern used to describe the linear orientation of multiple internal border zone infarcts located parallel to the lateral ventricles.11
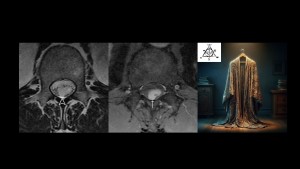
Invisibility cloak sign: This sign is a new proposal by our work team. On MRI, spinal schwannomas can be hyperintense on T2 and have a similar signal compared to the cerebrospinal fluid,12 and therefore not be evidently visible, demonstrating only indirect signs such as root displacement. This is reminiscent of a person hidden under a cloak of invisibility, something classically seen in famous fantasy novels.
Thoracic segment
Boot-shaped heart: It’s the appearance of the heart in patients with tetralogy of Fallot. The boot shape is produced by upturning of the cardiac apex because of right ventricular hypertrophy and by the concavity of the main pulmonary artery.13

Finger in glove: It refers to the description of bronchiectasis filled with respiratory secretions, resembling a finger in a glove. It’s classically associated with allergic bronchopulmonary aspergillosis. It can also be recognized in cystic fibrosis, asthma and obstructive diseases.3
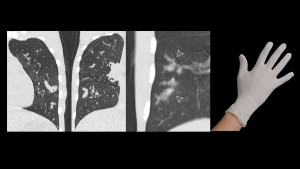
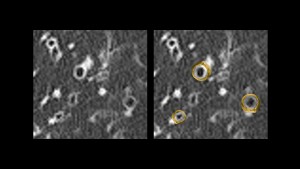
Signet ring (bronchiectasis): It’s seen on chest CT and refers to the appearance of a dilated bronchus, which exceeds the diameter of the adjacent pulmonary artery. The dilated bronchus represents the hollow of the ring, and the pulmonary artery the signet.3
Abdomen and pelvis
Beaded collar (primary sclerosing cholangitis): On MR Cholangiopancreatography (MRCP), primary sclerosing cholangitis can manifest as multi-focal segmental strictures of intra and extrahepatic bile ducts, producing a beaded appearance.3

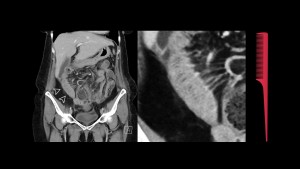
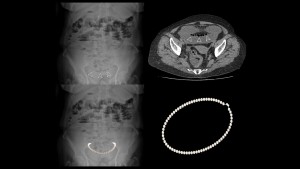
String of pearls (small bowel obstruction): In small bowel obstruction when there’s a lot of accumulated fluid, small bubbles appear separated by valvulae conniventes and can be seen as a chain of radiolucent images, which constitutes the string of pearls.14
Phrygian cap: It’s a common variant of the gallbladder which occurs when there’s folding of the fundus upon the gallbladder body. It remembers a hat worn by inhabitants of Phrygia.3

Comb sign (Crohn’s disease): It refers to fibrofatty proliferation and vascular dilation in active Crohn’s disease, giving the appearance of the teeth of a comb.3