Patients with abdominal aortic aneurysm (AAA) are treated with method of endovascular treatment of abdominal aortic aneurysms (EVAR) (Fig. 1). Even though, the EVAR grafting has started to become
the standard of care for abdominal aortic aneurysm repair over the past decades, the troubles related to long-term durability and necessities for re-intervention are still the worries of vascular specialists, who are performing EVAR technique in their patients with AAA every day around the world. Sometimes, vascular surgeons and interventional radiologists due to treatment of patients with increasingly hostile
iliac artery anatomies, need to look for abdominal stent-grafts specific for maintenance of iliac limb patency. Iliac limb occlusion or significant stenosis due to kinking caused by narrow iliac arteries, tortuous iliac vessels, or progressive aneurysmal degeneration are common complications of EVAR. The existence of narrow and tortuous iliac arteries is a major risk factor for limb kinking and thrombosis. Indeed, failure in limb patency may result in life-threatening ischemic complications, often necessitating urgent endovascular revascularization. Therefore, preoperative identification of adverse anatomy and careful stent graft selection before performing the EVAR technique are pivotal first steps to ensure favorable circumstances for the endovascular AAA treatment.
3D-printing technology has been used already to improve diagnosis and surgical treatment of complex vascular diseases. Previously, our group by Rynio et al. used a 3D-printing technology of abdominal aortic aneurysms and iliac arteries anatomic conditions for preoperative simulation before the personalized treatment of aortic lesions via physician-modified stent grafts (PMSG) that can be tailored to the specific vascular settings of the selected patients. Especially, it was useful in situations when a custom stent graft from the manufacturer took sometimes 12–15 weeks to be delivered, and the risk of rupture in symptomatic giant aneurysms was elevated. In this strategy, patients undergo regular Computed Tomography Angiography (CTA) in order to detect AAA size and iliac arteries aneurisms size and their treatment complications (Fig. 2). Certainly, CTA may offer the accurate way of assessing of anatomic conditions, such as the iliac tortuosity and kinking, and form the basis for surgical decision making before implantation of stent-graft (Fig. 3). However, there is possibility for physicians that they will encounter suboptimal or challenging anatomical conditions for a stent graft engraftment to the strongly bended iliac arteries (Fig. 4). Then, the standard method fails to detect some cases of incompatibility of stent graft design and real arterial geometry, which is challenging to predict based on CTA. Especially this occurs, when manufacturers of popular stent grafts do not unveil the exclusion criteria related to bends and twists in the iliac arteries. In this notion, the experimental simulation using the three-dimensional printed models of iliac artery angulations could be the more realistic technique performed in order to find the optimal stent-graft type and size, depending on the patient-specific anatomical geometry of vessels.
Hence, this study aimed to evaluate the use of ultrasound imaging technique with the purpose to analyze quantitatively the influence of different stent grafts’ shape designs on the hemodynamic parameters of tested stent grafts.
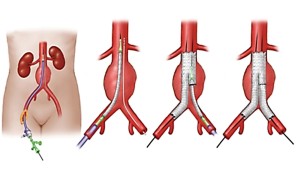
Fig. 1 Idea of the method of endovascular treatment of abdominal aortic aneurysm (EVAR) and iliac arteries vascular abnormalities, including severe kinks.
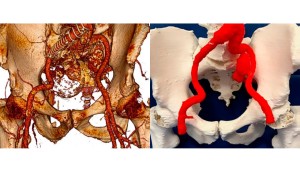
Fig. 2 Assessment of endoleak type II due to internal iliac artery aneurysm. Three-dimensional volume reconstruction of a CTA of a patient with endoleak to internal iliac artery aneurysm (left panel). Three-dimensional printed model of internal iliac artery aneurysm with endoleak (right panel). Modified from Rynio et al., J. Clin. Med. 2020, 9, 686.

Fig. 3 Angio-CT angulated iliac arteries before implantation of stent-graft.

Fig. 4 CTA of angulated iliac arteries after stent-graft implantation.