A nodule is currently defined as a circumscribed opacity less than or equalto 30 mm in average diameter and larger than 6 mm.
A rounded lesion less than 6 mm in diameter should be called micronodule.The latest Fleischner Glossary of Terms seeks to standardize the description and reporting of nodules:
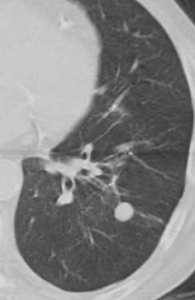
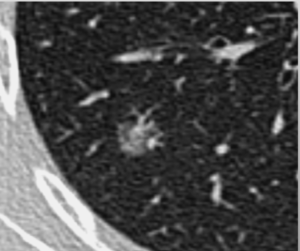
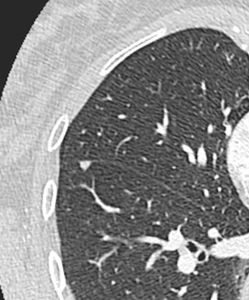
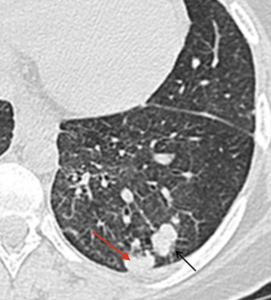
- Shape and Margins: Nodules can be described as round (Fig1), ovoid, or polygonal in shape, with margins that may be well-defined (fig1) or ill-defined. Irregular borders can be lobulated or spiculated and linear structures extending from the nodule to the pleura are called “pleural tags” (fig2).

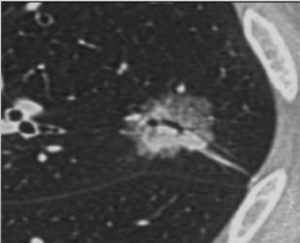
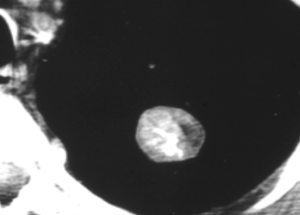
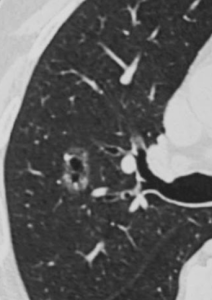
- Attenuation and Structure: Nodules with purely ground-glass attenuation are referred to as "ground-glass" nodules (fig3), while those with pure soft tissue attenuation are termed "solid" nodules. Nodules containing both ground-glass and soft tissue components are called “part-solid” nodules (Fig4).
Based on structure, nodules are classified as either “simple” or “complex.” Simple nodules consist of a single structural component (such as soft tissue, ground-glass, calcium, or fat), while complex nodules have two or more structural components.
-Location: Nodules can be categorized as peribronchovascular or centrilobular, depending on their position relative to other structures. Nodules originating from a fissure should be called “fissural”, while those in contact with, but not arising from a fissure should be labeled “perifissural.” Nodules originating from the pleura are termed “pleural” and those in contact with, but not arising from, the pleura are defined as “pleura-based”. The term “subpleural” should only refers to nodules that are near the pleura without direct contact.
The prefix "juxta" has been inconsistently used to describe nodules near or in contact with the pleura or a fissure (e.g., juxtafissural or juxtapleural). The Fleischner Glossary suggests using the more specific terminology described above instead.
After describing a pulmonary nodule using the precise terms outlined earlier, we can identify a higher risk of malignancy in nodules exhibiting features such as spiculation, pleural retraction, pleural thickening, the bronchus or vessel sign (where an airway or vessel leads directly to the lesion), and part-solid characteristics.
Furthermore, subsolid lesions that can be accompanied by pseudocavitation can be indicative of adenocarcinoma lesions.
In addition, ground-glass pulmonary nodules have a probability of malignancy of 10% to 50% when they persist beyond 3 months and are larger than 10 mm in diameter.
Finally, the Fleischner Society did not release new management recommendations for pulmonary nodules, maintaining those published in 2017, which are based on performing a high-resolution, low-dose chest CT.