PATHOPHYSIOLOGY OF COLONIC VOLVULUS
Volvulus can be defined as a twist between 180° to 360° around a transition point, which usually result in obstruction. Theoretically, for a volvulus to occur, a long and redundant colon segment with poor peritoneal fixation and the thinning of mesentery with a lead-point is necessary. This lead point, serving as the site of rotation, can be an adhesion or an intraluminal or extraluminal mass. This pathophysiology acts as a predisposing factor in elderly patients with multiple comorbidities. Colonic dysmotility, due to chronic constipation or laxative use in those patients, leads to elongation and subsequent dilatation of the colon, hence creating redundancy and making the bowel prone to torsion.
PRESENTATION
Twisting of sigmoid mesentery up to 180° is considered physiological. Torsion beyond 180° may lead to complications including bowel obstruction, ischemia, or necrosis with perforation.
Patients with volvulus may present with symptoms of a lower bowel obstruction including abdominal distention, nausea, vomiting, intermittent colicky diffuse abdominal pain, and constipation. It may have an insidious onset with vomiting before the onset of pain.
Late presentations may end up with sepsis or end-organ damage including hypotension, acute kidney injury leading to decreased urine output and altered mental status.
IMAGING OF VOLVULUS
Common initial workup to suspected bowel obstruction starts with an abdominal X-ray to identify pneumoperitoneum or obstruction.
CT is extremely beneficial in the diagnosis of sigmoid volvulus. It does not only confirm the diagnosis, but also help the assessment of the viability of the involved bowel loops using contrast enhancement.
Patients with any signs of perforation on imaging should be taken immediately to the surgery.
CLASSIC X-RAY FINDINGS:
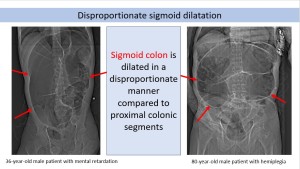
Disproportionate sigmoid dilatation: Sigmoid colon gets dilated disproportionately when compared to the proximal colonic segments (Fig. 1).
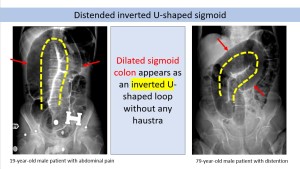
Distended inverted U-shaped sigmoid: The inverted dilated sigmoid loop without any haustral pattern in the shape of an inverted “U” extends into the right upper quadrant (Fig. 2).
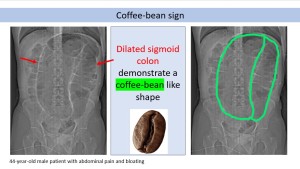
Coffee-bean sign: This sign refers to the coffee-bean like shape of the dilated sigmoid colon on abdominal plain radiographs (Fig. 3). It is also known as “kidney bean sign” or “bent inner tube sign”. The apposition of the medial walls of the dilated loop of bowel forms the cleft of the bean and lateral walls form the outer walls of the bean. It can be seen in both sigmoid and cecal volvulus.
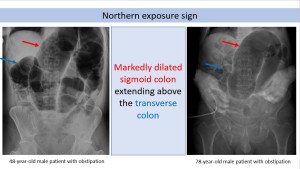
Northern exposure sign: It refers to the repositioning of the dilated sigmoid colon out of the pelvis and extension above the transverse colon. It is specific to sigmoid volvulus (Fig 4).
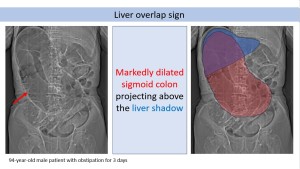
Liver overlap sign: It describes the cephalad positioning of the dilated sigmoid colon to the right upper quadrant, projecting over the liver shadow (Fig. 5).
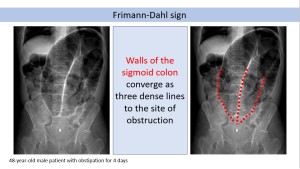
Frimann-Dahl sign: It describes the convergence of three dense lines, representing the walls of sigmoid, to the site of obstruction (Fig. 6).
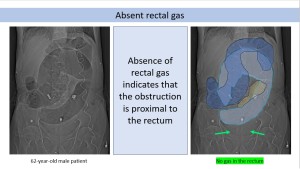
Absent rectal gas: Due to obstruction proximal to the rectum, gas is not seen in the rectum on plain radiographs (Fig. 7).
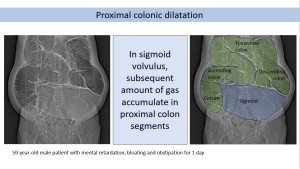
Proximal colonic dilatation: When the sigmoid volvulus presents as a closed loop obstruction, there may be substantial amount of gas in the more proximal colon and the small bowel (Fig. 8).
Abdominal X-rays may be limited in case the closed loop is fluid-filled, oriented anteroposteriorly or obscured by the loops of air distended bowel. CT of the abdomen and pelvis is usually obtained if the patient is clinically stable.
CT FINDINGS:
Closed loop obstruction: It describes a large gas-filled bowel loop without haustra.
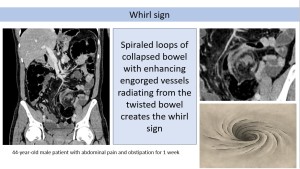
Whirl sign: It indicates the twisting of the sigmoid mesentery, which can be depicted on coronal and sagittal reformatting (Fig. 9). The appearance of spiraled loops of collapsed bowel with enhancing engorged vessels radiating from the twisted bowel often shows the point of obstruction. For unknown reasons, the swirling preferentially occurs in the counterclockwise direction in 70% of cases.
Bird beak sign: A beak-like tapering may be seen at the level of twisting of the sigmoid colon, both proximally and distally, and it may be confirmed with rectal contrast enema studies (Fig. 10).

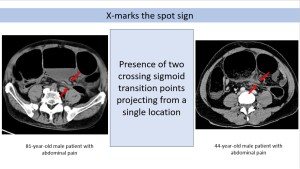
X-marks the spot sign: It identifies the presence of two crossing sigmoid transition points projecting from a single location (Fig. 11).
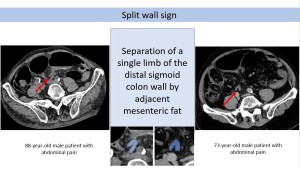
Split wall sign: It describes the apparent separation of a single limb of the distal sigmoid colon wall by adjacent mesenteric fat secondary to incomplete twisting or folding of the bowel loop. In this case, the single loop assumes a bilobed or C shape (Fig. 12).
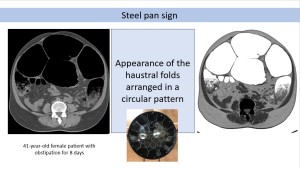
Steel pan sign: It describes the appearance of the haustral folds arranged in a circular pattern in the CT imaging with close resemblance to the Caribbean percussion instrument known as the steel pan or drum (Fig. 13).
SUBTYPES OF SIGMOID VOLVULUS
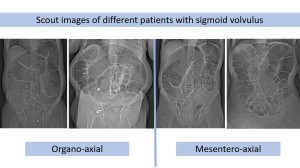
There are two main mechanisms of torsion in sigmoid volvulus according to the rotation axis of the colon: mesentero-axial and organo-axial (Fig.14). Abdominal plain radiographs are usually not sufficient to understand the type of the volvulus and usually CT scan is needed (Fig. 15).
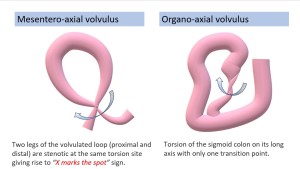
- Mesentero-axial sigmoid volvulus: In this type, the colon rotates around the axis of mesentery and causes a closed-loop obstruction where both ends of the loop get close together (Fig 16). The whirl sign, demonstrating the convergence of both limbs of the twisted bowel towards a fulcrum point, is commonly seen in the left lower quadrant. The loop of volvulated segment is typically very distended, lacks haustra and is located in the anterior part of abdomen.
 Fig 16: Mesentero-axial sigmoid volvulus
Fig 16: Mesentero-axial sigmoid volvulus - Organo-axial sigmoid volvulus: In this type, the colon rotates around the longitudinal axis of the bowel itself. Only a single transition point occurs and there is no closed loop obstruction (Fig. 17). A tight whirl sign, close to or at the rectosigmoid junction, may be seen and the upstream colon is usually dilated. Although closed loop obstruction is not seen, majority of organo-axial volvulus requires endoscopic or surgical intervention.
 Fig 17: Organo-axial sigmoid volvulus
Fig 17: Organo-axial sigmoid volvulus
There is also an extremely rare subtype of sigmoid volvulus known as ileosigmoid knotting. The ileum or sigmoid colon turns around the other segment. In this case, the strangulation of the sigmoid loop occurs as a result of winding of a small bowel loop around sigmoid but due to the rotation of the colon. It is also known as “compound”, “double loop” volvulus, or “gordion knot”.