Findings and procedure details
Biliary disorders can be classified on the basis of etiology and age at presentation. This poster reviews the spectrum of biliary disorders on the basis of age at presentation
Fig 1: Spectrum of biliary disorders on the basis of age at presentation
DISORDERS OF NEONATAL AGE GROUP
- BILIARY ATRESIA (BA)
This condition is characterized by deficient development of biliary tree. It has a female preponderance and syndromic association in 15-30% of cases. Three major anatomical types are recognized as per Kasai classification
Fig 2: Pictorial representation of the Kasai classification of biliary atresia. (a) Normal anatomy- green representing intrahepatic ducts, yellow- CHD, violet- cystic duct and blue- CBD. Color red represents obliteration of the segment.
Figure (b) shows a type 1 atresia, which involves obliteration of common bile duct (CBD) and cystic duct only. (c) Type 2a atresia involving common hepatic duct (CHD) with a patent CBD and cystic duct. (d) Type 2b atresia with involvement of the CBD, CHD and cystic ducts. (e) Type 3 atresia with obliteration of the left and right hepatic ducts.
Imaging Features
Ultrasound (USG)-
- Gall bladder (GB) ghost triad- Atretic GB <15 mm in length, irregular contour and a lack of smooth/ complete echogenic mucosal lining with indistinct wall. Lack of contractile GB is another feature
Fig 3: Biliary atresia in a 24 day old female with conjugated hyperbilirubinemia. Grey scale USG images (a and b) demonstrate a small gall bladder which has an irregular lobulated contour with echogenic walls (white arrows). The mucosal lining additionally appears to markedly irregular (yellow arrows). These features in conjugation are termed as the ‘ghost triad’.
(c and d) USG images in another patient of biliary atresia show absence of normal contractility of gall bladder after feeding.
- Triangular cord sign- presence of echogenic soft tissue>4 mm anterior to portal vein
Fig 4: (a and b) Triangular cord sign in a case of Biliary atresia in a 13 day old neonate with obstructive jaundice. Grey scale USG images of the liver (a and b- without and with annotation respectively) demonstrate increased echogenic soft tissue anterior to right portal vein ( EARPV, yellow calipers), which measured ~5.2 mm in this case. Increased echogenicity is also seen anterior to portal bifurcation. This sign is referred to as the triangular cord sign (TCS) and is representative of the atretic bile duct. (c) USG image additionally shows a small irregular GB, which measured 12 mm (marked with a caliper). (d) Elastography image shows increased parenchymal stiffness of the liver parenchyma with a mean stiffness 58.4 kPa (normal- <5.3 kPa).
Doppler and Elastography-
- Enlargement of hepatic artery >1.5 mm
- Hepatic subcapsular flow
- Increased parenchymal stiffness
Hepatic Scintigraphy-
- Can differentiate BA from other pathologies
- Uses 99mTc iminodiacetic acid (HIDA)
- Absence of radiopharmaceutical agent in the bowel is suggestive of BA
- Disadvantages- requires 5 Days of pre-treatment, has a high false positive rate and delays diagnosis by upto a week
MRCP - best reserved as a problem-solving modality due to cost and need for sedation. It is highly sensitive and specific (99% and 95% respectively) for diagnosis
Fig 5: (a) Axial T2 W MR image in a patient with biliary atresia shows the MR equivalent of TCS, visible as increased T2 hyperintense soft tissue at portal bifurcation (arrow, a) with non visualization of biliary radicals. (b) Hepato-iminodiacetate scan (HIDA) at 24 hours shows no visualization of the tracer in bowel, thereby strengthening the diagnosis of biliary atresia which was eventually confirmed intra-operatively.
Percutaneous Transhepatic / Intraoperative Cholangiogram is gold standard for diagnosis of BA and remains an alternative to prevent unnecessary surgery.
Cystic biliary atresia is a unique entity which needs to be differentiated from choledochal cysts
Fig 6: Table demonstrating the differentiating features between cystic biliary atresia and Choledochal cyst
Fig 7: Cystic biliary atresia in a neonate which was initially misdiagnosed as Choledochal cyst. (a and b) Grey scale USG images show a well defined thin walled oval anechoic cystic lesion at porta hepatis (asterisk). Gall bladder was not visualized. Additionally, there is absence of IHBRD with increased echogenicity at portal bifurcation (yellow arrow, a). Coronal (c, d) and axial (e and f) T2 W MR images confirm cystic dilatation of the CBD (black asterisk) with absence of IHBRD, suggesting the diagnosis of cystic biliary atresia over a Choledochal cyst.
CHOLEDOCHAL CYSTS
These represent cystic dilatation of the biliary tree due to a developmental alteration. Choledochal cysts are more often associated with anomalous pancreaticobiliary junction in form of a long common channel (>10 mm in length).
Todani classification is most commonly utilized to differentiate the morphological subtypes into 5 major categories. Isolated cystic duct dilatation has been added as type VI category within this classification
Fig 8: Pictorial representation of Todani’s classification of Choledochal cysts. (a) Normal anatomy- green representing intrahepatic ducts, yellow- CHD, violet- cystic duct and blue- CBD. Color red represents the pathologically dilated segment.
(b) Type I choledochal cyst, representing dilatation of the extrahepatic bile duct dilatation. (c) Type II cyst, which is diverticulum from extrahepatic bile duct. (d) Type III or choledochocoele, which represents focal dilatation of intramural segment of CBD. (e) Type IV a cyst, representing dilatation of both extra and intrahepatic biliary tree. (f) type IV b, consisting of multiple extrahepatic cysts only and (g) Type V, characterized by involvement of intrahepatic bile ducts only, also referred to as Caroli’s disease.
(h) A new entity of type VI cyst has also been added, where the dilatation is restricted to the cystic duct only.
On USG, these lesions appear anechoic /hypoechoic at porta hepatis anterior to portal vein. They show communication with biliary tree and are separate from the gall bladder, which is normal in these patients
Fig 9: Type IVa Choledochal cyst with cholangitis in a 3 year old female with fever, right upper quadrant pain and jaundice. (a-c) Grey scale and doppler USG images demonstrate gross cystic dilatation of right and left hepatic ducts with IHBRD and fusiform dilatation of the CBD. There is additional presence of avascular internal echogenic contents (asterisks) within the dilated biliary system with mural wall thickening (arrow, c).
(d-f) Serial axial T2 W MR images confirm the extra and intrahepatic biliary involvement with T2 hyperintense mural wall thickening in CBD (arrow) and a long common channel (yellow arrow, f). Coronal T2 (g) and MRCP projection (h) confirm the presence of a dilated anomalous pancreatico-biliary junction with a long common channel (LC, h) after the union of CBD and pancreatic duct (PD).
Scintigraphy, whenever done shows radiotracer excretion into the cyst.
MRCP remains the investigation of choice in delineating the morphology and distribution, detecting presence of concomitant anomalous pancreaticobiliary duct union and complications like stone and cholangiocarcinoma
Fig 10: (a-d) Type 1 Choledochal cyst in a 15 year old with abdominal pain and dilated CBD on USG. Serial axial (a, b) and coronal (c) T2W MR images show fusiform dilatation of extrahepatic bile duct with mild central IHBRD, which is likely due to stasis. MRCP image (d) shows involvement of CHD and CBD with a small signal void s/o calculus with sludge at the lower end of CBD (arrow).
(e) Type 1 Choledochal cyst in a 2 year old female. MRCP image shows saccular dilatation of CBD with relative preservation of the caliber of intrahepatic ducts.
(f) Type VI Choledochal cyst in a 7 year old patient. MRCP projection shows isolated dilatation of the cystic duct (arrow).
CAROLI’S DISEASE
This congenital disorder is characterized by multifocal cystic dilatation of segmental intrahepatic bile ducts and is now recognized as a separate entity related to ductal plate malformation. There are described associations with congenital hepatic fibrosis and autosomal recessive polycystic kidney disease (ARPKD).
USG shows multiple dilated intrahepatic ducts surrounding the portal vein radicals
CT and MRI show ‘central dot sign’ representing dilated intrahepatic ducts with enhancing central dots within, representing corresponding portal radical. MRCP shows continuity of the cysts with biliary tree
Fig 11: Caroli’s disease with autosomal recessive polycystic kidney disease (ARPKD) in a newborn with conjugated hyperbilirubinemia. (a) Grey scale USG image focused at liver show multiple anechoic thin walled intrahepatic cysts with central echogenic portal radical (arrow). (b and c) USG of renal fossa shows an enlarged echogenic right kidney (b) which is due to numerous tiny cysts, as observed on the image focused with a linear transducer (arrows, c).
(d-f) Axial T2 W MR images in another patient with Caroli’s disease show multiple T2 hyperintense intrahepatic cysts, predominantly in right lobe (d and e) with few showing debris within. On MRCP image (f), the cysts show communication with the biliary tree.
CONGENITAL BILIARY WEB AND STRICTURE
Developmental webs and strictures form a rare cause of intrahepatic and/or extrahepatic CHD/CBD obstruction. There are associated with conditions like choledochal cysts and congenital hepatic fibrosis.
Both have a predilection towards involvement of bile duct bifurcation. USG is non-specific and shows IHBRD. MRCP and ERCP are superior in demonstrating areas of involvement
Fig 12: Congenital biliary web in a 1 month female with jaundice. (a-c) Serial axial T2 W MR and MRCP (d) images demonstrate significant dilatation of the right, left hepatic ducts and bilobar IHBRs with an abrupt truncation after the cystic duct unites with the CHD (arrow). There is non visualization of the CBD distally.
INSPISSATED BILE SYNDROME
This self-limiting condition is a rare cause of mechanical biliary obstruction in neonates and is caused due to plugging of extra-hepatic bile ducts with biliary sludge.
USG shows echogenic sludge within bile duct lumen without shadowing with upstream dilatation of biliary tree
Fig 13: Inspissated bile syndrome in 13 day male with conjugated hyperbilirubinemia. (a-b) Grey scale ultrasound image (a) shows presence of echogenic sludge without shadowing within the lumen of common bile duct with no significant vascularity on Doppler (b).
Upstream biliary tree dilatation helps in differentiation of this entity from biliary atresia.
BILE DUCT HAMARTOMAS
Hamartomas of the biliary system, also known as Von-Mayerberg complexes, occur due to failure of involution of embryonic bile ducts. They are asymptomatic and are incidentally detected on imaging.
On USG, these appear as tiny hyperechoic lesions with comet tail artifacts.
CT and MRI show multiple small hypoattenuating cysts. They can be confused with simple cysts however bile duct hamartomas are much more numerous, are smaller and have uniform size (<1.5 cm) with irregular outline.
On MRCP images, they do not show any communication with biliary tree
Fig 14: Bile duct hamartomas in a patient being evaluated for pancreatitis. Axial (a) and coronal (b) T2 W images show numerous small cysts scattered in both lobes of liver. On MRCP image (c), the cysts show no communication with the biliary tree.
DISORDERS PRESENTING BEYOND NEONATAL AGE GROUP
PRIMARY SCLEROSING CHOLANGITIS (PSC)
PSC is a chronic progressive immune mediated biliary disorder characterized by inflammation of bile ducts with consequent fibrosis and destruction. Involvement can be both intrahepatic and /or extrahepatic in nature. PSC is relatively rare in children, however is observed in association with ulcerative colitis. Cirrhosis as the end result develops within 1 to 10 years.
Imaging with USG shows echogenic tissue surrounding portal venules and ducts with irregular multisegmental bile duct dilation.
CT shows discontinuous biliary dilatation with biliary wall thickening at porta hepatis and reactive lymphadenopathy.
MRCP is diagnostic and shows pruning of the peripheral ducts with alternating strictures and dilatation in the bile ducts, giving a beaded appearance. Skip lesions are common and IHBRD is usually minimal
Fig 15: PSC in a 15 year old female with ulcerative colitis and obstructive jaundice. Grey scale USG image (a) shows echogenic mural wall thickening in CBD at porta hepatis (solid arrow). Serial axial CECT images (b) show dilated biliary radicles (solid arrows). MRCP projection (c) demonstrates marked pruning or progressive narrowing (arrow heads) of the peripheral bile ducts with ‘beaded’ appearance of the biliary tree due to alternating biliary strictures (white arrows) and dilated intervening segments (yellow arrows). ERCP image (d) confirms the pruned appearance (arrow heads) of the peripheral biliary tree with dilatation of the central ducts. Significant intrahepatic and extrahepatic involvement (arrows) is demonstrated.
ERCP is gold standard and shows beading, pruned tree appearance with mural irregularity and diverticulae.
IgG4 SCLEROSING CHOLANGITIS
IgG4 related disease in another immune mediated multi-systemic disease characterized by fibro-inflammatory lesions rich in IgG4 positive plasma cells and elevated serum IgG4 levels. Bile duct involvement occurs in about 60-80 % cases.
Although both intra and extra-hepatic biliary system can be involved like PSC, there is a particular predilection for hilar and intrapancreatic CBD involvement.
MRI typically shows circular, symmetric T2 hypointense rind of soft tissue encasing the CBD wall with smooth margins and delayed homogeneous enhancement
Fig 16: IgG4 related sclerosing cholangitis in a 14 year old female with IgG4 level of 2.3 g/l (upper limit for normal levels -1.35 g/l). Serial axial (a, b) and coronal (c) T2 W images show dilatation of the bilobar IHBRs with a dilated CBD (arrow, b and c). MRCP image (d) demonstrates multiple hilar strictures (arrows, d). Axial (e) and Coronal (f) post contrast images in delayed phases show circumferential concentric homogeneously enhancing soft tissue around CBD (yellow arrows, e and f) and PD (white marrow, e) with resultant luminal attenuation.
Fig 17: Pictorial representation of the various imaging features of (a) Primary sclerosing cholangitis and (b) IgG4 related cholangitis. Red ovals in (b) represent the frequent areas of involved segments.
BILIARY ASCARIASIS
Ascaris lumbricoides is the most frequent helminthic infection to affect the biliary tract and is a result of migration of the worms from the intestine to CBD.
While majority of the infestations are asymptomatic, patients can present with painless jaundice.
USG shows linear or tubular echogenic intraductal structures with or without dilatation.
MRCP- Worms appear as a linear hypointense defect within the bright CBD. Occasionally, a ‘Three line sign” representing a central hyperintense line in between two hypointense lines is characteristic, with the central line representing worm gut
Fig 18: Biliary ascariasis in a 4 year old male. Grey scale USG images (a and b) show multiple tubular echogenic structures within the right and left hepatic ducts (arrows, a and b) with no significant dilatation. Axial T1 W (c) and T2W (d) images show intraductal linear lesions appearing T1 hyperintense (arrow, c) and T2 hypointense (arrow, d). Serial MRCP projections (e and f) show multiple linear serpiginous signal voids within the right, left hepatic ducts and confluence (arrows).
LANGERHANS CELL HISTIOCYTOSIS (LCH)
Hepatobiliary involvement in LCH is observed less than 20% of patients and is common in multicentric disease. Imaging features are a result of infiltration of the periportal space by Langerhans cells.
There are four characteristic histopathological stages of involvement and show varying imaging features.
(1) Proliferative and (2) granulomatous stages show enhancing periportal tissue on CT and MRI with the periportal hyperintensity on T2W images representing periportal oedema.
(3) Xanthomatous stage is characterised by deposition of Lipid-laden nodules in liver. These appear hyperechoic on US, hypoattenuating on CT and hyperintense on unenhanced T1-weighted MRI.
[4] Final fibrous stage shows advanced features in form of biliary cirrhosis and secondary portal hypertension.
Direct histiocytic infiltration of bile ducts results in secondary sclerosing cholangitis with consequent intra- and extrahepatic biliary irregularities, formation of bile lakes and areas of focal narrowing and dilatation
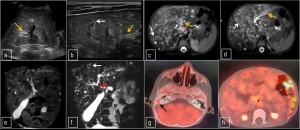
Fig 19: Langerhans cell histiocytosis with biliary involvement in a 3 year old boy with abdominal distention, hepatomegaly and jaundice. Gray scale USG images (a and b) show hyperechoic sheet like periportal thickening extending along the biliary radicals (yellow arrows). Few anechoic cysts were also observed (white arrow, b). On serial axial T2W MR images (c and d), hyperintense periportal thickening (yellow arrows) with numerous cysts are seen in both lobes showing a preferential peribiliary distribution (white arrows) and are representative of bile lakes consequent to the obstructive biliary thickening. A dominant stricture is additionally observed at hilum (red arrow) with upstream biliary dilatation. Enlarged retroperitoneal nodes are also noted (asterisk). Coronal T2 W (e) and MRCP image (f) show no communication of the cysts. Axial fused 18 fluoro-deoxy-glucose (FDG) PET-CT images at the level of mastoid bone (g) and abdomen (h) show a mildly avid lytic lesion involving right mastoid bone (black arrow) with increased tracer uptake within retroperitoneal nodes (asterisk, h).
Fig 20: LCH related hepatobiliary involvement in a 3 year old. Axial CECT image (a) shows hypodense periportal soft tissue (white arrow) with ill defined hypoattenuating areas in right lobe of liver (yellow arrow). Serial axial (b, c) and coronal (d, e) T2W MR images confirm the hyperintense periportal thickening (white arrows) with confluent T2 hyperintensity in right lobe and multiple additional lesions in segment 3 of liver (yellow arrows). MRCP image (f) shows the multifocal irregular strictures within the right sided biliary tree (yellow arrows) with dilated left hepatic duct. Another stricture is seen in the common hepatic duct just proximal to cystic duct insertion (white arrow).
PORTAL BILIOPATHY
Extra hepatic portal venous obstruction (EHPVO) can occasionally lead to biliary obstruction. This may occur due to mechanical obstruction by collaterals or formation of strictures in extrahepatic part of biliary tree secondary to collaterals.
CT and MRI typically show cavernomatous transformation with encasement of biliary system by collaterals and IHBRD
Fig 21: (a-c) Portal biliopathy in a 10 year old male with EHPVO and post splenectomy. Serial axial (a, b) and coronal (c) CECT images show replacement of the portal vein by multiple collaterals which are encasing biliary tree (yellow arrows, b and c) with upstream mild central IHBRD (white arrow, a).
(d-f) Biliary dilatation due to fibrotic stricture associated with long standing EHPVO in a 17 year old male. Serial axial T2W images (d and e) show portal cavernoma formation (white arrows) with biliary sludge in gall bladder and gamma gandy bodies (yellow arrow). MRCP image (f) demonstrates consequent gross biliary dilatation involving intrahepatic ducts and CHD.
MRCP can demonstrate extrinsic mass effect on biliary system with smooth tapering of hepatic ducts or localized sacculations.
BILIARY RHABDOMYOSARCOMA (RMS)
Also known as sarcoma botryoides, embryonal variant of RMS is the most common paediatric biliary tumour.
The average of onset is 4yrs with females being affected twice as males. CBD is most commonly involved and the tumour may masquerade initially as choledochal cyst with sludge.
Immuno-histochemical analysis is useful in diagnosis of embryonal RMS as >95 % are positive for desmin.
USG shows markedly distended CBD filled with soft tissue and upstream biliary dilatation.
CT and MRI demonstrate an enhancing variable signal intraductal mass within the distended duct and assist in preoperative staging
Fig 22: Biliary RMS in a 7-year-old boy with obstructive jaundice, hepatomegaly and deranged liver enzymes. Serial axial CECT images (a, b) demonstrate gross expansion of the extrahepatic bile duct with an intraluminal heterogeneous mass (arrows). The GB is also markedly distended due to distal bile flow obstruction. Percutaneous transhepatic cholangiography (PTC) image (c) shows a distended CBD with a large ovoid filling defect.


 Fig 3: Biliary atresia in a 24 day old female with conjugated hyperbilirubinemia. Grey scale USG images (a and b) demonstrate a small gall bladder which has an irregular lobulated contour with echogenic walls (white arrows). The mucosal lining additionally appears to markedly irregular (yellow arrows). These features in conjugation are termed as the ‘ghost triad’. (c and d) USG images in another patient of biliary atresia show absence of normal contractility of gall bladder after feeding.
Fig 3: Biliary atresia in a 24 day old female with conjugated hyperbilirubinemia. Grey scale USG images (a and b) demonstrate a small gall bladder which has an irregular lobulated contour with echogenic walls (white arrows). The mucosal lining additionally appears to markedly irregular (yellow arrows). These features in conjugation are termed as the ‘ghost triad’. (c and d) USG images in another patient of biliary atresia show absence of normal contractility of gall bladder after feeding. Fig 4: (a and b) Triangular cord sign in a case of Biliary atresia in a 13 day old neonate with obstructive jaundice. Grey scale USG images of the liver (a and b- without and with annotation respectively) demonstrate increased echogenic soft tissue anterior to right portal vein ( EARPV, yellow calipers), which measured ~5.2 mm in this case. Increased echogenicity is also seen anterior to portal bifurcation. This sign is referred to as the triangular cord sign (TCS) and is representative of the atretic bile duct. (c) USG image additionally shows a small irregular GB, which measured 12 mm (marked with a caliper). (d) Elastography image shows increased parenchymal stiffness of the liver parenchyma with a mean stiffness 58.4 kPa (normal- <5.3 kPa).
Fig 4: (a and b) Triangular cord sign in a case of Biliary atresia in a 13 day old neonate with obstructive jaundice. Grey scale USG images of the liver (a and b- without and with annotation respectively) demonstrate increased echogenic soft tissue anterior to right portal vein ( EARPV, yellow calipers), which measured ~5.2 mm in this case. Increased echogenicity is also seen anterior to portal bifurcation. This sign is referred to as the triangular cord sign (TCS) and is representative of the atretic bile duct. (c) USG image additionally shows a small irregular GB, which measured 12 mm (marked with a caliper). (d) Elastography image shows increased parenchymal stiffness of the liver parenchyma with a mean stiffness 58.4 kPa (normal- <5.3 kPa).















