Results
In total, 147 participants were included of which 37 (25%) had pathologically confirmed ENE+ nodes.
Fig 5: Table 2: The demographic and clinical information of the 147 participants in the development dataset
Note.—Unless otherwise indicated, data are numbers of participants, with percentages in parentheses. ENE = extranodal extension.
* Data are mean ± SD.
Fig 6: Figure 4: Flowchart showing the inclusion and exclusion criteria for the development dataset and validation cohort. TME = total mesorectal excision, DWI = diffusion-weighted imaging, b-LN = benign lymph node, ENE- LNM = metastatic lymph nodes without ENE, ENE+ LNM = metastatic lymph nodes with ENE, TD = tumor deposit.
In the univariable analysis, only the ratio of short- to long-axis diameter and the relative distance were not different between pathologic-ENE- and pathologic-ENE+ nodes.
Fig 7: Table 3: Univariable and multivariable analyses of MRI characteristics potentially associated with extranodal extension in the development dataset
Note.—Unless otherwise indicated, data are numbers of nodes, with percentages in parentheses. ENE = extranodal extension, SAD = short-axis diameter, LAD = long-axis diameter, CSE = chemical shift effect.
a Mann‒Whitney U test; b χ2 test. * Data are median (interquartile range). † Data in parentheses are 95% CIs.
The interobserver agreements of all categorical characteristics were moderate to almost perfect (κ values range, 0.46-0.85). Of these, the agreements for the two novel characteristics, i.e. broken-ring sign and tail sign, were both substantial, with kappa values of 0.67 and 0.66, respectively. And the long-axis diameter was excluded from the multivariable analysis for its strong correlation between the short-axis diameter.
Multivariable logistic regression analyses indicated that the heterogeneous internal structure and the presence of the broken-ring sign and tail sign independently contributed to the detection of ENE on MRI.
Fig 7: Table 3: Univariable and multivariable analyses of MRI characteristics potentially associated with extranodal extension in the development dataset
Note.—Unless otherwise indicated, data are numbers of nodes, with percentages in parentheses. ENE = extranodal extension, SAD = short-axis diameter, LAD = long-axis diameter, CSE = chemical shift effect.
a Mann‒Whitney U test; b χ2 test. * Data are median (interquartile range). † Data in parentheses are 95% CIs.
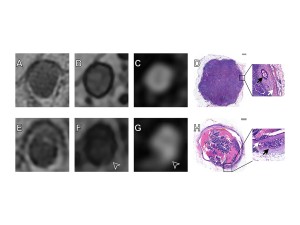
Fig 8: Figure 5: MRI scans and photomicrograph of two representative nodes. (A - D) Images of a metastatic lymph node without extranodal extension in an 85-year-old female with rectal cancer. (A) Axial T2-weighted imaging shows homogeneous structure within the node. (B) Axial opposed-phase T1-weighted imaging shows a complete and continuous sharp black circle surrounding the node, that is, the absence of a broken-ring sign. (C) Axial diffusion-weighted imaging (DWI) with b = 0 shows the node as isolated and sharply defined with high signal and no other high signal around, indicating the absence of a tail sign. (D) Hematoxylin and eosin staining shows the node is a metastatic lymph node without extranodal extension. In the enlarged image (magnification, ×20), the white arrow points at the capsule, and the black arrow points at the tumor. (E - H) Images of a metastatic lymph node with extranodal extension in a 57-year-old male with rectal cancer. (E) Axial T2-weighted imaging shows a heterogeneous structure within the node. (F) Axial opposed-phase T1-weighted imaging shows the sharp black circle surrounding the node is interrupted (arrowhead), indicating the presence of a broken-ring sign. (G) Axial DWI with b = 0 shows that a band-like high signal appeared around the node and was directly attached to the node (arrowhead), indicating the presence of a tail sign. (H) Hematoxylin and eosin staining shows the node is a metastatic lymph node with extranodal extension. In the enlarged image (magnification, ×20), the white arrow points at the capsule, and the black arrow points at the tumor.
Fig 9: Figure 6: Diagnostic flowchart for detecting extranodal extension (ENE) on pretreatment MRI. Any node in the mesorectum or around the superior rectal artery with the interruption of vessels, fusion, or broken-ring sign on MRI was directly classified as MRI detected ENE+ without further analysis. Nodes that did not meet these criteria were assessed for internal structural heterogeneity and the presence of the tail sign on MRI and were classified as MRI detected ENE+ when both characteristics were present; otherwise, they were classified as MRI detected ENE-.
The established process showed an excellent diagnostic performance to preoperatively detect ENE, with an AUC, sensitivity, specificity, PPV, NPV and accuracy of 0.91, 88%, 94%, 60%, 99%, and 93%, respectively.
Fig 10: Figure 7: Receiver operating characteristic (ROC) curves of the weighted linear combination, the process and three independent factors, that is the internal structure, broken-ring sign, and tail sign, for the detection of extranodal extension.
A total of 110 patients with locally advanced rectal cancer were included in the validation cohort (Fig 6). After a median follow-up of 37 months, 16 (46%) of the 35 patients with MRI-detected ENE presented in pretreatment MRI experienced disease progression, compared with 8 (11%) of the 75 patients without MRI-detected ENE.
Kaplan-Meier survival curves and log-rank test combined with multivariate Cox analysis showed that MRI-detected ENE (hazard ratio [HR], 3.00 [95% CI: 1.17, 7.71]; P = .02) was one of the independent factors indicating poorer 3-year DFS.
Fig 11: Table 4: Multivariable Cox regression analyses for 3-year disease-free survival by baseline clinical data and MRI characteristics in the validation cohort
Note.— NAT = neoadjuvant therapy, EMVI = extramural venous invasion, ENE = extranodal extension.
* Data are numbers of patients, with percentages in parentheses. † Data in parentheses are 95% CIs.





