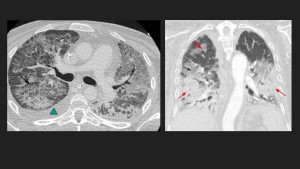
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS)
Acute respiratory distress syndrome (ARDS) is the term applied to a spectrum of conditions with different etiologies sharing common clinical-pathological features, including:
- Increased permeability of the alveolo-capillary membrane, resulting in inflammatory edema
- Increased non-aerated lung tissue, resulting in higher lung elastance (lower compliance)
- Increased venous admixture and dead space, which result in hypoxemia and hypercapnia

There are several risk factors that may end up developing an acute respiratory distress syndrome:

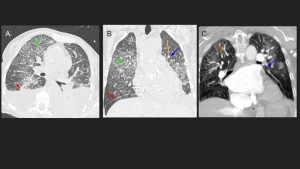
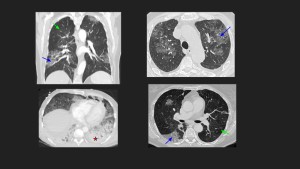
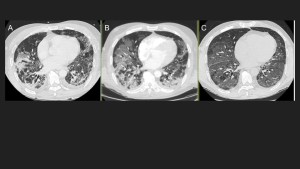
Radiological findings (see also Table 2):
- Bilateral heterogeneous ground-glass opacities and consolidations
- Interlobular septal thickening
- Symmetric or asymmetric lung involvement
- Pleural effusions less common than in cardiogenic pulmonary edema
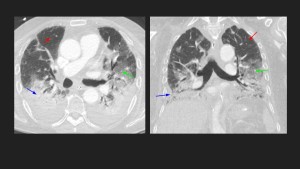
ACUTE CARDIOGENIC PULMONARY EDEMA
Accumulation of excessive fluid in the alveolar walls and alveolar spaces of the lungs caused by elevated pulmonary capillary pressure originating from a cardiac impairment.
Pathophysiology: ↑ pressure/fluid accumulation → ↑ pulmonary venous pressure → ↑ pulmonary capillary pressure → fluid in interstitial spaces → ↑ pressure in interstitial spaces → fluid in alveoli
Clinical manifestations:
Characteristics of left, right or simultaneous ventricular failure:
- Dyspnea, orthopnea and paroxysmal nocturnal dyspnea
- Tachypnea and tachycardia
- Jugular venous distention and peripheral edema
- Pink frothy sputum
- Angina
- Cool and clammy skin
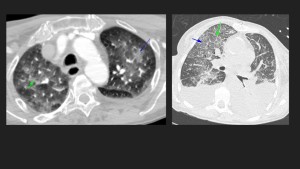
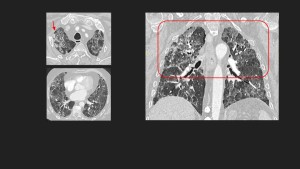
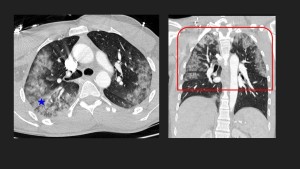
Radiological findings:
- Central ground-glass opacities with peripheral area preservation ("bat wing" alveolar edema)
- Inter and intralobar septal thickening
- Peribronchial cuffing
- Cardiomegaly
- Bilateral pleural effusions and thickening of fissures
- Consolidation
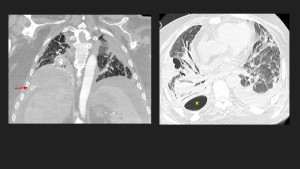
PULMONARY HEMORRHAGE
It represents blood extravasation into alveoli due to multiple pathologies. Can be diffuse or localized.
Distribution may be:
- Diffuse: Vasculitis, Goodpasture syndrome, coagulation disorders, hemosiderosis, etc.
- Localized: Vasculitis, pulmonary infarction, infectious, traumatic, neoplastic, AVM, iatrogenic, etc.
Clinical manifestations:
- Hemoptysis
- Complementary tests: hypoxemia
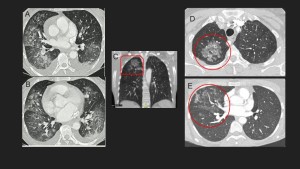
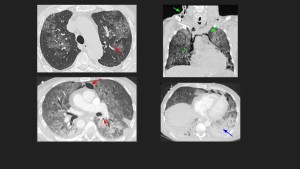
Radiological findings:
Diffuse:
- Widespread ground-glass opacification with septal thickening (crazy paving pattern)
- May associate with areas of consolidation
Localized:
- Ground-glass opacity limited to an area of lung parenchyma
PNEUMOCYSTIS JIROVECI
Pneumocystis jirovecii pneumonia is a potentially fatal opportunistic fungal disease commonly affecting immunocompromised patients (HIV, immunosuppressants, biological agents, corticosteroids, hematologic malignancies, solid tumors, etc).
Clinical manifestations:
- Dyspnea
- Non-productive cough
- Fever
- Complementary tests: hypoxemia, PCR (+), BAL (cysts), CD4 lymphocyte count < 200 mm3
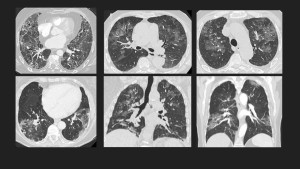
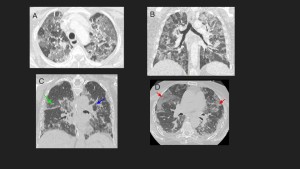
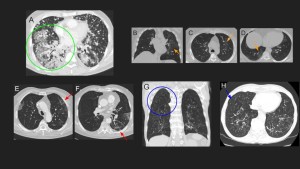
Radiological findings:
- Ground-glass pattern (main finding)
-
- Perihilar or upper/mid-zones (main involvement)
- Peripheral area preservation (~40%)
- Bilateral or asymmetric opacities
- Septal thickening or reticular opacities ("crazy paving" pattern)
- Pneumatoceles (~30%) predominantly involving the upper lobes. Higher risk of spontaneous pneumothorax and pneumomediastinum
- Atypical features: consolidation, nodules and "tree-in-bud" opacities suggesting an intercurrent infectious bronchiolitis, pleural effusion and adenopathy
BACTERIAL AND VIRAL PULMONARY INFECTIONS
Pulmonary infection caused by microorganisms (bacteria or viruses) presenting a diverse array of clinical manifestations and varying degrees of seriousness
Clinical manifestations of bacterial infection:
- Fever (>38°C)
- Productive cough with purulent sputum
- Dyspnea, tachypnea and increased respiratory effort
- Complementary tests: hypoxemia, leukocytosis, urine antigen test (+), blood/respiratory cultures (+)
Radiological findings of bacterial infections:
- Consolidation (heterogeneous density) associated with air/fluid bronchogram
- Ground-glass opacity
- Nodules: diffuse or patchy tree-in-bud suggestive of bronchiolitis
- Abscesses
- Empyema: infected purulent and often loculated pleural effusion


Clinical manifestations of viral infection:
- Low-grade fever
- Flu-like symptoms or upper respiratory tract infection signs
- Non-productive cough
- Dyspnea, tachypnea and increased respiratory effort
- Complementary tests: hypoxemia, PCR tests (+)
Radiological findings of viral infections:
- Altered lung parenchymal attenuation with heterogeneously patchy areas (mosaic pattern)
- Ground-glass opacities
- Interlobular septal thickening (crazy paving pattern)
- Nodules/micronodules and tree-in-bud opacities
- Thickening of bronchial/bronchiolar walls
- Consolidation and fibrotic pattern evolution
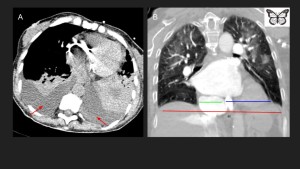
ACUTE ASPIRATION PNEUMONIA / PNEUMONITIS
Lung injury associated with the aspiration of solid and/or liquid materials into the airways and lungs. Clinical manifestations and radiological findings will depend on the type of content and the severity of the aspiration.
Clinical manifestations:
- Cough
- Purulent sputum
- Hemoptysis
- Fever
Radiological findings:
Posterior segments of the upper lobes and superior segments of the lower lobes are frequently involved when patients aspirate in recumbent position, whereas the bibasilar segments, right middle lobe, and lingular segment are affected in erect patients.
- Centrilobular nodules with tree-in-bud pattern → Impaction of aspirated particles in distal airways.
- Ground-glass opacities (parenchymal inflammation)
- Central airway obstruction
- Segmental or lobar atelectasis
- Consolidations which can associated air/fluid bronchogram

DRUG-INDUCED LUNG DISEASE
Lung injury resulting from different types of agents (antineoplastics, anti-inflammatories, cardiovascular agents, antibiotics, etc.), presenting with various clinical manifestations and severity.
It is a diagnosis of exclusion.
Clinical and radiological improvement may occur upon discontinuation of therapy.
Nonspecific clinical manifestations:
- Dyspnea
- Non-productive cough
- Fever
- Complementary tests: hypoxemia, eosinophilia
Radiological findings:
- Ground-glass alveolar or interstitial opacities (reticular and/or nodular opacities).
CRYPTOGENIC ORGANIZING PNEUMONIA (COP)
Cryptogenic organizing pneumonia (COP) is a form of diffuse idiopathic interstitial lung disease resulting from alveolar injury triggering an inflammatory and fibroproliferative process, characterized by fibrotic plugs within alveoli obstructing alveolar and bronchiolar lumens. Interstitial inflammation and fibrosis are minimal or absent.
The idiopathic form has no identifiable cause, meanwhile, the secondary form can be caused by a wide range of infectious/non-infectious causes.
Reversible with immunosuppressive or anti-inflammatory therapy.
Clinical manifestations:
- Acute dyspnea (rapidly progressive forms)
- Non-productive cough
- Dry crackles
- Fever
- Complementary tests: hypoxemia, increased inflammatory markers (ESR, C- reactive protein and leukocytes)
Radiological findings:
- Peripheral or peribronchial bilateral patchy migratory consolidations and ground-glass opacities
- Atoll or reversed halo sign: ground-glass opacities surrounded by a peripheral consolidation
- Bronchial dilatation (it may reproduce an air bronchogram sign within a consolidation or ground-glass opacity)
- Perilobular pattern: bowed or polygonal opacities with poorly defined margins bordering the interlobular septa (specific finding)
- Nodular or reticular opacities
- Fibrotic pattern


