Result
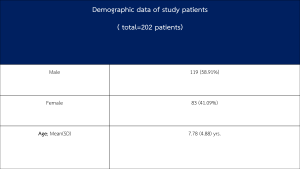
Demographic data
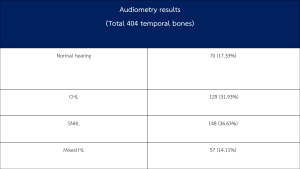
Total populations were 202 patients or 404 temporal bone CTs. A total of 404 audiometry results (temporal bones) comprising normal hearing, CHL, SNHL, and mixed HL were 70 (17.33%), 129 (31.93%), 148 (36.63%), and 57 (14.11%) respectively as Table 2,3.
Prevalence of cochlear cleft and extent
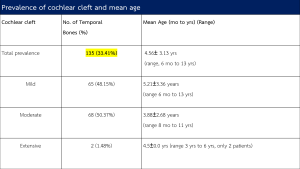
This study found 33.41% (135 of a total 404 temporal bones) of cochlear cleft in children with and without hearing loss. Mean age for cochlear cleft group was 4.56±3.13 years (range, 6 months to 13 years) as Table 4. In cochlear cleft group (n= 135), moderate degree was the most frequent involvement pattern (n= 68, 50.37%). Mild degree was found in 65 temporal bones (48.15%), while an extensive degree was found in only 2 temporal bones (1.48%). Mean ages for mild, moderate, and extensive groups were 5.21±3.36 years(range 6 months to 13 years), 3.88±2.68 years (range 8 months to 11 years), and 4.5±0.0 years(range 3 years to 6 years, only 2 patients), respectively (Table4).
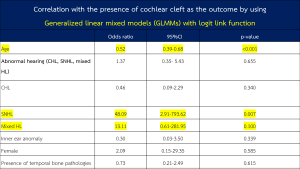
Correlation with presence of cochlear cleft as the outcome by using Generalized linear mixed models (GLmms) with the logit link function.
For presence of cochlear cleft as the outcome, age, SNHL, mixed HL, and temporal bone malformation were associated with a p-value of 0.20 or less, and considered for the backward stepwise analysis (Table 5).
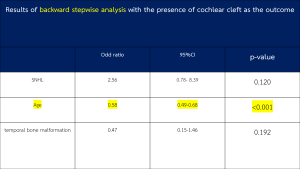
Results of backward stepwise analysis with presence of cochlear cleft as the outcome In backward stepwise for the presence of cochlear cleft as the outcome, only age was statistically significantly related to presence of cochlear cleft( p-value<0.001),as table 6
Correlation between presence of cochlear cleft and each age group
“Liu’s method” provided optimal cutoff point for each age group into 0-4 years old, 5- 8 years old, and >8 years old groups. Correlation was found between presence of cochlear cleft and younger age groups (0-4 and 5-8 years, p-value <0.001 and 0.019, respectively) as Table 7.

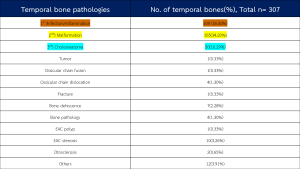
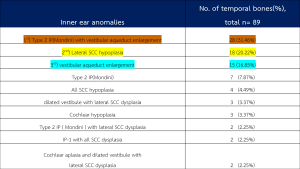
Prevalence of temporal bone pathologies and inner ear anomalies The prevalence of total temporal bone pathologies was 75.99% (307/404temporal bones). While three most common temporal bone pathologies were infection/inflammation (109/307 temporal bones, 35.50%), malformation (105/307 temporal bones, 34.20%),and cholesteatoma (50/307 temporal bones, 16.29%) respectively. Various inner ear abnormalities were observed in 89/404 (22.03%) temporal bones. Most common inner ear abnormality was incomplete partition type 2 with vestibular aqueduct enlargement (n=28, 31.46%). In descending order of frequency, other inner ear abnormalities such as lateral semicircular canal hypoplasia (n=18, 22%) vestibular aqueduct enlargement (n=15, 85%), etc. as shown in table 8,9
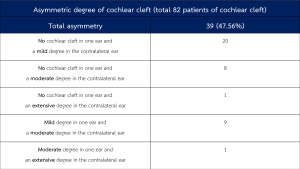
Prevalence of cochlear cleft asymmetry Extent of cochlear cleft was asymmetric between two ears of the same patient in 39 of 82 cases(47.56%) , most with asymmetric degree of cochlear cleft (20 patients) showed no cochlear cleft in one ear, while the other ear presented a mild degree. In 9 patients, asymmetric degree of cochlear cleft was a mild degree in one ear and a moderate degree in contralateral ear.Another 8 patients with asymmetric degree of cochlear cleft were no cochlear cleft in one ear and a moderate degree in the other. In the remaining 2 patients, asymmetric degree was moderate and extensive degrees in 1 patient, and in another one were no cochlear cleft and extensive degrees. as Table 10.
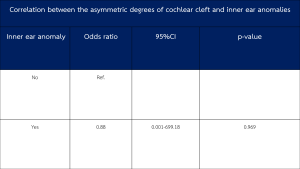
Correlation between presence of cochlear cleft and inner ear anomalies
In 9 of 39 patients presenting with asymmetric degree of cochlear cleft, various inner ear anomalies were found. Inner ear structures were radiologically normal in the remaining 30 patients with asymmetric degree of cochlear cleft.The asymmetric degree did not have a statistically significant correlation with underlying inner ear anomalies(P=0.969) as Table 11.