The US LIRADS algorithm consists of an ultrasound category and a visualization score, both assigned to the entire examination.
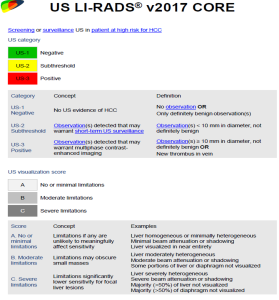
Ultrasound category :
The ultrasound category is applied to the liver as a whole rather than individual lesions. It is determined based on the most suspicious finding observed. The US LIRADS algorithm includes three categories:
US-1 Negative:
Studies classified as US-1 include those with no suspicion of malignancy, such as:
- A normal examination with no detected observations.
- An examination showing benign observations based on sonographic appearance (e.g., cysts, focal fat infiltration) or previously characterized as benign using other diagnostic modalities such as hemangioma.
- An examination with observations previously classified sub-threshold and proven stable after serial follow-ups over two years may be downgraded to US-1.
 Fig 3: Focal lesion previously diagnosed as haemangioma by contrast enhanced CT. (definitely benign observation)
Fig 3: Focal lesion previously diagnosed as haemangioma by contrast enhanced CT. (definitely benign observation)
An examination may include findings requiring further evaluation but carries no suspicion for HCC, such as intrahepatic biliary dilation. Although further workup may be recommended, the study remains categorized as US-1.
US-1 is a negative study, recommended to continue routine screening after six months.
US-2 subthreshold
This category includes solid observations that are not definitively benign, such as nodules of any echogenicity measuring less than 1 cm in their longest dimension.
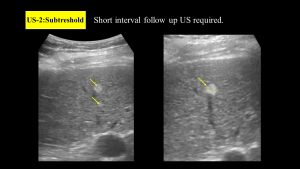
The size threshold of less than 1 cm was chosen as a cut off measurement as characterization of nodules less than 1 cm is not feasible on any contrast enhanced modality. Short-term follow-up is required within 3 to 6 months, continuing for up to 2 years. If the nodule remains stable, it may be reclassified as US-1. However, if its size increases beyond 1 cm, malignancy is strongly suspected, necessitating further evaluation with a diagnostic contrast-enhanced imaging modality
US-3 Positive
This category includes studies with suspected malignancy that require further characterization, such as:
- Solid observations larger than 1 cm.
- Areas of focal parenchymal heterogeneity greater than 1 cm, which may present as architectural distortion.
- Thrombus in the portal or hepatic vein.
 Fig 5: Examples of positive examinations: areas of parenchymal heterogeneity (A), focal solid observations(more than 1 cm) (B) and new portal vein thrombus (C) .(Not definitely benign).
Fig 5: Examples of positive examinations: areas of parenchymal heterogeneity (A), focal solid observations(more than 1 cm) (B) and new portal vein thrombus (C) .(Not definitely benign).
Size is the primary determinant for follow-up recommendations, regardless of echogenicity. These findings require further evaluation using a contrast-enhanced imaging modality.
In cases of uncertainty when assigning a US category, the observer should choose the category with the higher level of suspicion to ensure timely and appropriate follow up.
Visualization score
It is assigned based on the degree to which the entire liver can be assessed and is used to evaluate the quality of the ultrasound examination.
Visualization score is affected by both intrinsic and extrinsic factors:
- Intrinsic factors are related to liver characteristics, such as severe fatty changes that hinder ultrasound beam penetration, making it difficult to visualize deeper liver structures. Advanced cirrhosis with significant parenchymal heterogeneity can also obscure underlying masses. Additionally, volume dysmorphism and global atrophy may further impair a comprehensive liver assessment.
- Extrinsic factors include rib shadowing, obesity, gaseous distention, and ascites, all of which can limit visualization.
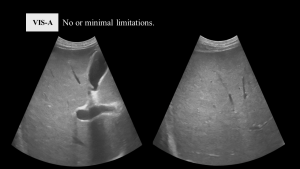
Visualization score A (VIS A) No or minimal limitations:
It is an examination with no significant limitations affecting the detection sensitivity of focal lesions, ensuring complete and confident visualization of the entire liver. Minimal limitations may be present but do not compromise the examination’s accuracy.
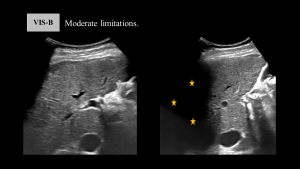
Visualization score B (VIS B) Moderate limitations:
Assigned for examinations with moderate limitations that affect the assessment of the entire liver and may obscure sub-centimeter lesions; however, still considered diagnostically acceptable.
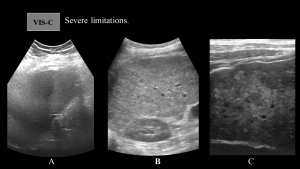
Visualization score C (VIS C) Severe limitations:
This examination has severe limitations, significantly hindering the assessment of large focal lesions or more than half of the liver volume. It is crucial to document the reasons for limited visualization, whether due to intrinsic factors (such as liver-related changes that obscure focal lesions) or extrinsic factors (which impede visualization of more than 50% of the liver parenchyma). Since extrinsic limitations may improve in subsequent ultrasound studies, repeating the examination should be considered before proceeding with a contrast-enhanced diagnostic modality.
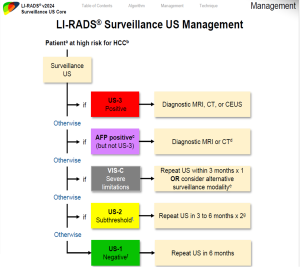
In v2017, the management plan relied on the ultrasound category. In v2024, the algorithm was updated to incorporate AFP levels and VIS-C score. Patients with positive AFP now undergo contrast-enhanced CT or MRI, even if their ultrasound findings are negative. Additionally, alternative imaging modalities are considered for patients with VIS-C score.