The peritoneum
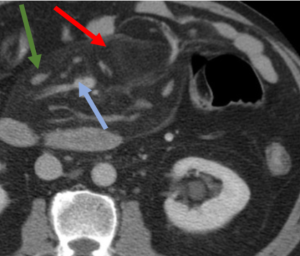
The presence of ascites or contrast in the peritoneal cavity helps define its anatomical boundaries:
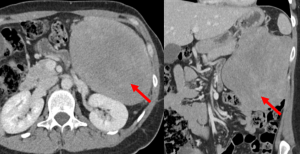
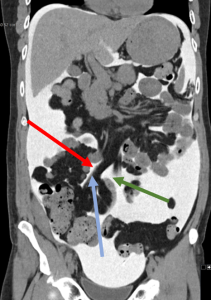
- The anterior parietal peritoneum (red arrows) is inseparable from the anterior abdominal wall. The posterior parietal peritoneum (blue arrows) anteriorly delineates the kidneys and the rectum (retroperitoneal organs).
 Fig 1: CT axial slice demonstrating the anterior and posterior borders of the peritoneum
Fig 1: CT axial slice demonstrating the anterior and posterior borders of the peritoneum - The uterine round ligaments (red arrows), which are covered by peritoneum, form the lateral margins of the pelvis in women, extending from the uterine fundus to the inguinal canal.
 Fig 2: CT axial slice at the pelvic level demonstrating the round ligaments delimitating the lateral borders of the peritoneal cavity
Fig 2: CT axial slice at the pelvic level demonstrating the round ligaments delimitating the lateral borders of the peritoneal cavity -
The rectovesical pouch (blue arrow) in men, and the douglas pouch/rectovaginal recess in women represent the most caudal extension of the peritoneal cavity.
 Fig 3: CT sagittal slice demonstrating the rectovesical space in a man (blue arrow), located behind the bladder (red arrow).
Fig 3: CT sagittal slice demonstrating the rectovesical space in a man (blue arrow), located behind the bladder (red arrow).
The abdominal cavity can be divided into two major spaces: the greater sac and the lesser sac.They communicate with each other through the epiploic foramen (also known as the foramen of Winslow).
The Peritoneal Cavity
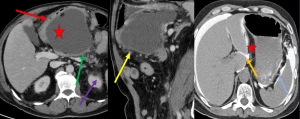
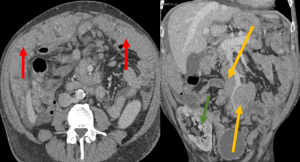
The peritoneal cavity can be subdivided into the supramesocolic space (red arrow) and the inframesocolic space (blue arrow), by the transverse mesocolon (illustrated by the green line).
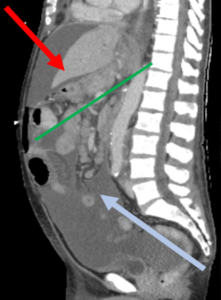
The transverse mesocolon is continuous with the greater omentum (which surrounds the transverse colon) and extends posteriorly, where it becomes the transverse mesocolon. It splits anterior to the duodenum, enveloping the pancreas and the retroperitoneal organs, prior to attaching to the posterior abdominal wall.It contains the middle colic artery and vein, and lymphatic vessels.
The Greater Omentum
The Greater Omentum, or Epiploon, derives from the Latin word "apron." It extends from the greater curvature of the stomach to the anterior transverse colon and covers the small intestine. In healthy individuals we are not able to see it, however due to its intraperitoneal location is a very frequent site for metastatic deposits ("omental cake"), most commonly by gastric of ovarian cancers.

Supramesocolic Compartment:
The Supramesocolic compartment can be further subdivided into right and left supramesocolic spaces. They are in continuity with each other and can be further subdivided into smaller compartments:
Right supramesocolic space
The right supramesocolic compartment can be subdivided into 3 spaces:
- Subhepatic space
- Subfrenic space
- Lesser sac
Right Subhepatic compartment:
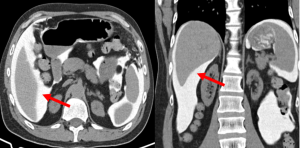
The right subhepatic space, also known as the Morrison's pouch (red arrow), is located between the inferior surface of the liver and the upper pole of the right kidney. Due to its dependent location, it is a frequent place of blood products accumulation (ie. from hepatic trauma or iatrogenic causes).
Right Subhepatic compartment:
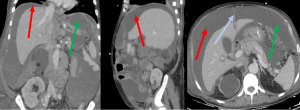
The right subphrenic space (red arrow) is located between the inferior surface of the right diaphragm and the superior surface of the right hepatic lobe. It is separated incompletely from the left supramesocolic space (green arrow) by the falciform ligament (blue arrow).
Lesser Sac:
The lesser sac or omental bursa is the potential space formed by the lesser and greater omentum. Its only visible when filled, usually by collections (from pathologies affecting the pancreas, transverse colon, stomach or caudate lobe).
The lesser sac is bordered:- Anteriorly by the posterior wall of the stomach, the caudate liver lobe and the greater omentum; - Posteriorly by the pancreas and left kidney;- Lateraly by the Foramen of Winslow and the left gastrosplenic ligament;- Superiorly by the inferior surface of the liver;
Left Subhepatic compartment:
The left supramesocolic space can be subdivided into 2 subspaces:
-
Left subphrenic space (red arrow):Located between the inferior surface of the diaphragm and the superior surface of the liver (green arrow), gastric fundus (blue), and spleen (orange arrow).
 Fig 9: Left subphrenic space (red arrow)
Fig 9: Left subphrenic space (red arrow) -
Left subhepatic space (red arrow): Located between the stomach (blue arrow) and the left hepatic lobe (green arrow).
 Fig 10: Left subhepatic space (red arrow)
Fig 10: Left subhepatic space (red arrow)
Inframesocolic Space:The inframesocolic space is the compartment below the transverse mesocolon, and like its upper counterpart, it can also be divided into left and right by the mesentery of the small intestine, which extends obliquely from the duodenojejunal flexure (ligament of Treitz) to the ileocecal valve.As such, the contents of the right infracolic compartment have to pass anteriorly to the ileocecal valve to reach the pelvis, while the contents of the left infracolic compartment have a relatively longer route to the pelvis.
Paracolic gutters:
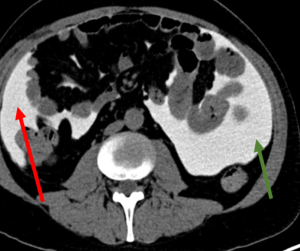
The paracolic gutters are peritoneal recesses located between the parietal peritoneum of the lateral abdominal walls and the ascending (right) and descending (left) colon.
Peritoneal Pathologies
Many pathologies can envolve the peritoneum.
The most common manifestation of pathologies involving peritoneum is ascites, that is accumulation of abnormal fluid in peritoneal cavity.
In the next section we will provide examples of some of the most common pathologies affecting the peritoneum in each categories.
Volvulus:
In Intestinal volvulus the bowel twists around its mesentery.

Inflammatory:
Omental infarts are a cause of acute abdominal pain and can mimic appendicitis, cholecystitis, or diverticulitisUsually are caused by torsion of a omental vein, leading to trombosis. On CT manifest as a focal area of fat densification with a peripheral hyperdense halo.Most common on the left iliac fossa.
Mesenteric Panniculitis:
Is a non-specific inflammation of the adipose tissue in the intestinal mesentery of unknown etiology. While most of them are of benign course, some authors describe an increased risk of developing lymphoma.Is also called as "Misty Mesentery"- as it manifest as increased density of the mesentery, with multiple prominent mesenteric lymph nodes.
Neoplasms:
Peritoneal Carcinomatosis:
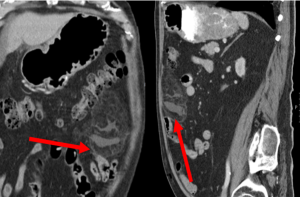
Spread of tumors to the peritoneal cavity, usually by direct invasion (seeding) from different organs (most common from cancers affecting the stomach, ovaries and colon). Correct and complete description of the location and size of the peritoneal implants are of extreme importance for treatment and surgical planning.Usually manifests as nodular thickening and enhancement of peritoneal folds (arrow) and/or nodules with soft tissue densities and Omental Caking.
Peritoneal Lymphomatosis (PL):
Its a relatively rare manifestation of Non-Hodgkin lymphoma (NH), manifesting as intraperitoneal dissemination of lymphomaOn Ct it manifest as a homogeneous thickening of the peritoneum or bulky masses which can mimic peritoneal carcinomatosis.
While the differentiation sometimes can be challenging, is of utmost importance, since carcinomatosis usually is treated with surgical excision of the implants (when possible), while peritoneal lymphomatosis is usually treated conservatively with chemotherapy.Some aspects that helps the radiologist making the distintion between them is that PL usually presents with disseminated adenomegalies and bulky implants, while CP presents with smaller adenomegalies (usually more regional) and smaller peritoneal nodules.
Pseudomyxoma Peritonei
Defined as the presence of mucinous/gelatinous thick ascites along peritoneal surfaces, caused by a primary mucinous neoplasm (usually from the appendix). It can cause mass effect on the different abdominal organs, like the liver), mesenteries, and small intestine.

Desmoid Tumor:
Its a tumor composed of non-inflammatory fibroblastic tissue.
Despite being a benign tumor, it is locally aggressive and presents a high risk of recurrence after surgical resection
Approximately 40% originate in the root of the mesentery; abdominal wall, retroperitoneum and typically affects young women (between 20-40 years).Can occur spontaneously or associated with Gardner syndrome or after local trauma/surgeryIt presents as a well-defined, homogeneous mass, which is isodense or with a slight enhancement compared to muscles.