Ethical committee approval was obtained for this retrospective study. Institutional PACS and RIS reports were searched between December 2020 and June 2024. The inclusion criteria for patient selection were as follows:
- Age: 18–99 years
- Signed written informed consent
- MR imaging including at least two fluid-sensitive sequences in two different planes and one T1-weighted turbo spin-echo (TSE) sequence
- The term "acute muscle injury" stated in the report summary
Exclusion criteria included incomplete examinations and non-diagnostic imaging quality. All patients were scanned in the supine position using one of the following institutional scanners: 1.5 Tesla (Sola, Avanto, Aera; Siemens Healthcare, Erlangen, Germany) or 3.0 Tesla (Vida, Skyra; Siemens Healthcare, Erlangen, Germany).
Readout
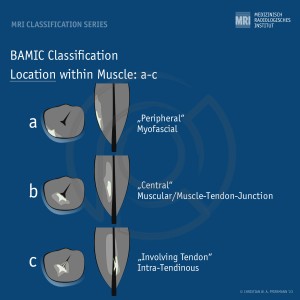
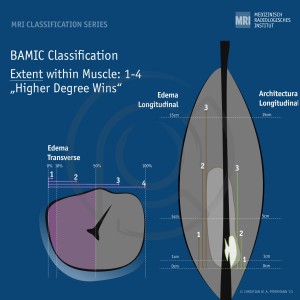
All images were classified using all three classification systems (for details, see Figures 1-5) by four fellowship-trained musculoskeletal radiologists (SF with 12 years, KH with 12 years, ABR with 19 years, and CWAP with 27 years of experience in MSK imaging). Each radiologist was blinded to the initial MRI report and to the readout results of the other readers.



Statistics
Study data were collected and managed using REDCap® electronic data capture tools (Version 13.5.4; Vanderbilt University, USA), hosted at the Schulthess Clinic, Zurich, Switzerland.
Inter-reader agreement was quantified using Fleiss’ Kappa with an associated 95% confidence interval. Kappa values were classified as poor (Kappa < 0), slight (0 ≤ Kappa ≤ 0.20), fair (0.21 ≤ Kappa ≤ 0.40), moderate (0.41 ≤ Kappa ≤ 0.60), substantial (0.61 ≤ Kappa ≤ 0.80), and almost perfect (0.81 ≤ Kappa ≤ 1.00).
Patient characteristics are presented as mean and standard deviation or as absolute and relative counts. The analysis was conducted using MATLAB (The MathWorks Inc., Version 2022b, Natick, Massachusetts)