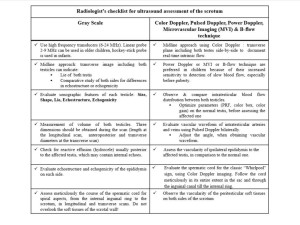
Ultrasound examination is the mainstay for the assessment of an acute scrotum. Moreover, performing US-assisted manual testicular detorsion has been documented in current literature [7].It is highly recommended that a brief history should be taken before the ultrasound exam, as the clinical correlation of findings is crucial for the final diagnosis. Figure 2 presents a detailed technique for testicular sonography.
According to Bandakar et al., there are three key sonographic findings for testicular torsion [1].
1. “Whirlpool sign”
The “whirlpool sign” represents an abrupt change to the course of the spermatic cord due to the spiral “torsion knot,” located mostly at the external inguinal ring or inside the scrotal sac [1].
2. Redundant spermatic cord
A redundant spermatic cord is defined as the presence of tortuous spermatic cord in the scrotal sac, usually at the external inguinal ring, hence raising suspicion for high attachment of the tunica vaginalis [1]. Normally, excess spermatic cord is not detected in the scrotal sac [1].
In torsion, the redundant cord usually seems like an extra-testicular, ovoid, heterogenous mass, often including epididymis at the superior aspect of the testis or inside the scrotal sac [1, 8]. Blood flow can be preserved in all or part of the redundant cord, depending on the degree of the torsion.
3. Horizontal or oblique lie
The normal testis lies vertically [1]. A transverse image of the normal scrotum reveals the testes side-by-side with the echogenic mediastinum directed posterolaterally [1]. A horizontal lie is attributed to the high attachment of the tunica vaginalis [9]. In the mid-testis transverse plane of the scrotum, the horizontal testis lies on its long axis and the normal one on its short axis [9]. When the testis lies in an oblique position, it is seen on a diagonal axis [10]. Additionally, a mediastinum testis with anteromedial direction is associated with torsion when presented with acute scrotal pain [11].
The different types of testicular torsion are illustrated through a series of cases evaluated in our Radiological Department. The sonographic findings are highly correlated with the degree of spermatic cord torsion, the onset of symptoms and whether the cord twist is tight or loose. Diagnosis of testicular torsion is based on a combination of findings on gray-scale and Color Doppler imaging.
Complete
Gray-scale imaging reveals:
- an enlarged spherical testis with altered lie [3, 12]. The testis and epididymis may occasionally present with normal echostructure and echogenicity during the first 2-4 hours [12]. However, scrotal parenchyma becomes gradually more hypoechoic and then hyperechoic with marked heterogenicity, while a swollen epididymis with heterogeneous echotexture, and hyperechogenicity is noted. [3, 12].
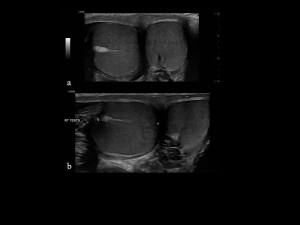
 Fig 6: Complete testicular torsion in a 10-year-old boy, who was admitted for acute pain in the left hemi-scrotum and nausea. a. Split gray-scale image (longitudinal and transverse plane) reveals a slightly enlarged left testicle, with normal echostructure and presence of multiple small non-shadowing hyperechoic foci within the testicular parenchyma, indicating testicular microlithiasis. Left testis (LT). b. Split gray- scale image (longitudinal and transverse plane) demonstrates a normal right testis, also with testicular microlithiasis. c. Longitudinal image with Microvascular technique shows absence of internal blood flow on the affected testis (left). Left testis (LT T).
Fig 6: Complete testicular torsion in a 10-year-old boy, who was admitted for acute pain in the left hemi-scrotum and nausea. a. Split gray-scale image (longitudinal and transverse plane) reveals a slightly enlarged left testicle, with normal echostructure and presence of multiple small non-shadowing hyperechoic foci within the testicular parenchyma, indicating testicular microlithiasis. Left testis (LT). b. Split gray- scale image (longitudinal and transverse plane) demonstrates a normal right testis, also with testicular microlithiasis. c. Longitudinal image with Microvascular technique shows absence of internal blood flow on the affected testis (left). Left testis (LT T). Fig 7: Complete testicular torsion in a 14-year-old boy, who presented with a painful left testicle for the past two days. a. Split gray-scale longitudinal and transverse image of left testicle demonstrates an enlarged with more spherical morphology, heterogenous left testicle, and hypogenic parenchymal fluid collections (arrow). A marked increase in the soft peritesticular tissues of the left hemi-scrotal wall (asterisk) is noted, due to edema. Left testis (LT TEST). b. Split gray-scale longitudinal and transverse image of a normal contralateral (right) testicle. Soft tissues surrounding the right testicle (asterisk) have a normal sonographic appearance, unlike Figure 1a. Right testis (RT TESTS). c. Color Doppler imaging shows lack of internal parenchymal flow.
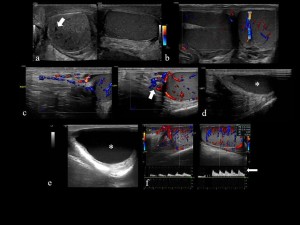
Fig 7: Complete testicular torsion in a 14-year-old boy, who presented with a painful left testicle for the past two days. a. Split gray-scale longitudinal and transverse image of left testicle demonstrates an enlarged with more spherical morphology, heterogenous left testicle, and hypogenic parenchymal fluid collections (arrow). A marked increase in the soft peritesticular tissues of the left hemi-scrotal wall (asterisk) is noted, due to edema. Left testis (LT TEST). b. Split gray-scale longitudinal and transverse image of a normal contralateral (right) testicle. Soft tissues surrounding the right testicle (asterisk) have a normal sonographic appearance, unlike Figure 1a. Right testis (RT TESTS). c. Color Doppler imaging shows lack of internal parenchymal flow. Fig 8: Complete testicular torsion in a 15-year-old boy who presented with testicular pain for the last ten days, following an incident of scrotal trauma during physical activity two weeks ago. a. Split gray-scale plane demonstrates an enlarged, rounded, heterogeneous right testis, with small cystic areas in the testicular parenchyma. Echogenic effusion is also documented. testis (RT TESTS). b. Gray-scale transverse image reveals effusion with multiple echogenic septa (arrow), indicating encysted effusion. testis (RT TESTS). c. Gray-scale longitudinal plane three days after exploratory surgery shows loss of normal shape of the right testis and heterogenous echostructure. d. Midline Color Doppler imaging confirms grayscale findings, as the right testicle shows no intratesticular blow flow, whereas cystic lesions indicate parenchymal necrosis. The left testicle shows normal vascularity. Right testis (RT).
Fig 8: Complete testicular torsion in a 15-year-old boy who presented with testicular pain for the last ten days, following an incident of scrotal trauma during physical activity two weeks ago. a. Split gray-scale plane demonstrates an enlarged, rounded, heterogeneous right testis, with small cystic areas in the testicular parenchyma. Echogenic effusion is also documented. testis (RT TESTS). b. Gray-scale transverse image reveals effusion with multiple echogenic septa (arrow), indicating encysted effusion. testis (RT TESTS). c. Gray-scale longitudinal plane three days after exploratory surgery shows loss of normal shape of the right testis and heterogenous echostructure. d. Midline Color Doppler imaging confirms grayscale findings, as the right testicle shows no intratesticular blow flow, whereas cystic lesions indicate parenchymal necrosis. The left testicle shows normal vascularity. Right testis (RT). - a reactive hydrocele with internal echoes posteriorly and inferiorly to the testis approximately six hours after the onset of pain [3, 12].
- a twisted course and swollen appearance of the spermatic cord; a “whirlpool sign” is sometimes identified [1, 10].
 Fig 9: Complete testicular torsion of left testis in a 14-year-old boy, who presented with 12 hours of right testicular pain and experienced nausea and vomiting along with the pain. a. Gray-scale transverse image in the midline shows both testicles. The right testis is more hyperechoic in comparison to the left one. b. Split gray-scale (longitudinal and transverse plane) of the right testis reveals an enlarged, spherical testis with a hyperechogenic and heterogenous sonographic appearance of its parenchyma. Free fluid (asterisk) is also present in the right hemi-scrotum. c. Color Doppler image demonstrates a spiral appearance (arrow) of the right spermatic cord in the intratesticular space. Free fluid (asterisk) is detected.
Fig 9: Complete testicular torsion of left testis in a 14-year-old boy, who presented with 12 hours of right testicular pain and experienced nausea and vomiting along with the pain. a. Gray-scale transverse image in the midline shows both testicles. The right testis is more hyperechoic in comparison to the left one. b. Split gray-scale (longitudinal and transverse plane) of the right testis reveals an enlarged, spherical testis with a hyperechogenic and heterogenous sonographic appearance of its parenchyma. Free fluid (asterisk) is also present in the right hemi-scrotum. c. Color Doppler image demonstrates a spiral appearance (arrow) of the right spermatic cord in the intratesticular space. Free fluid (asterisk) is detected. - thickened peritesticular soft tissues [12].
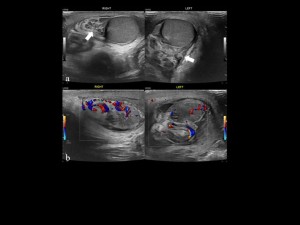
 Fig 10: Complete testicular torsion of left testis in a 14-year-old boy who presented with 3 days of groin pain on the left side. a. Gray-scale transverse image showing an enlarged, heterogeneous left epididymis. Left epididymis (LE) b. Color Doppler interrogation shows absent blood flow in the left epididymis, indicating participation in the torsion complex. c. Color Doppler image demonstrates an increased blood flow distribution in the periphery of left testicular parenchyma, whereas no blood flow is detected in the central zone (Halo sign). Left testis (LT) d. Gray-scale transverse image in the midline reveals enlargement of the soft peritesticular tissues of the ipsilateral hemi-scrotal wall. Skin thickening partially involves contralateral hemi-scrotum. Right testis (RT).
Fig 10: Complete testicular torsion of left testis in a 14-year-old boy who presented with 3 days of groin pain on the left side. a. Gray-scale transverse image showing an enlarged, heterogeneous left epididymis. Left epididymis (LE) b. Color Doppler interrogation shows absent blood flow in the left epididymis, indicating participation in the torsion complex. c. Color Doppler image demonstrates an increased blood flow distribution in the periphery of left testicular parenchyma, whereas no blood flow is detected in the central zone (Halo sign). Left testis (LT) d. Gray-scale transverse image in the midline reveals enlargement of the soft peritesticular tissues of the ipsilateral hemi-scrotal wall. Skin thickening partially involves contralateral hemi-scrotum. Right testis (RT).
Color Doppler imaging demonstrates:
- marked decrease or absence of intratesticular blood flow [3, 12].
- the “halo sign” , which consists of absent intratesticular blood flow and increased peripheral flow when the onset of sudden pain is greater than 24 hours [13]. Fig 10: Complete testicular torsion of left testis in a 14-year-old boy who presented with 3 days of groin pain on the left side. a. Gray-scale transverse image showing an enlarged, heterogeneous left epididymis. Left epididymis (LE) b. Color Doppler interrogation shows absent blood flow in the left epididymis, indicating participation in the torsion complex. c. Color Doppler image demonstrates an increased blood flow distribution in the periphery of left testicular parenchyma, whereas no blood flow is detected in the central zone (Halo sign). Left testis (LT) d. Gray-scale transverse image in the midline reveals enlargement of the soft peritesticular tissues of the ipsilateral hemi-scrotal wall. Skin thickening partially involves contralateral hemi-scrotum. Right testis (RT).
 Fig 11: Complete testicular torsion of left testis in a 13-year-old boy with 6 hours of acute scrotal pain, followed by a first attempt of detorsion maneuver in the emergency department. a. Split Color Doppler imaging reveals decreased blood flow in the central segment of the left testicular parenchyma. b. Split B-flow imaging confirms the findings of Color Doppler imaging. c. Split Color Doppler imaging after the second detorsion US-assisted maneuver shows that blood flow in the left testicle remains decreased. Right testis (RT), Left testis (LT).
Fig 11: Complete testicular torsion of left testis in a 13-year-old boy with 6 hours of acute scrotal pain, followed by a first attempt of detorsion maneuver in the emergency department. a. Split Color Doppler imaging reveals decreased blood flow in the central segment of the left testicular parenchyma. b. Split B-flow imaging confirms the findings of Color Doppler imaging. c. Split Color Doppler imaging after the second detorsion US-assisted maneuver shows that blood flow in the left testicle remains decreased. Right testis (RT), Left testis (LT). - increased, reduced blood flow or even avascular appearance of the epididymis [1, 13].
- increased blood flow of the affected testis, epididymis and cord, when followed by detorsion maneuver [7].
 Fig 12: Complete testicular torsion in a 12-year-old boy, who presented with acute left testicular pain, along with vomiting for the past two hours. a. Midline approach of the scrotum. Gray-scale image shows both testicles. The left testicle is slightly enlarged compared to the right one. However, parenchymal echogenicity seems similar on both sides. b. Color Doppler plane reveals increased blood flow to the epididymis, whereas absence of intratesticular blood flow is noted. c. Color Doppler image after US-assisted detorsion maneuver demonstrates a hyperemic elongated left spermatic cord, indicating successful manual detorsion. d. Color Doppler plane reveals increased blood flow on the left testicle and epididymis.
Fig 12: Complete testicular torsion in a 12-year-old boy, who presented with acute left testicular pain, along with vomiting for the past two hours. a. Midline approach of the scrotum. Gray-scale image shows both testicles. The left testicle is slightly enlarged compared to the right one. However, parenchymal echogenicity seems similar on both sides. b. Color Doppler plane reveals increased blood flow to the epididymis, whereas absence of intratesticular blood flow is noted. c. Color Doppler image after US-assisted detorsion maneuver demonstrates a hyperemic elongated left spermatic cord, indicating successful manual detorsion. d. Color Doppler plane reveals increased blood flow on the left testicle and epididymis. - marked vascularity of peritesticular soft tissues.
Partial
Gray-scale imaging shows:
- a symmetrically or asymmetrically affected testis to the contralateral one regarding size, position, echostructure and echogenicity [1]. Ηypechogenic lines within the scrotal parenchyma can be identified due to interstitial and septal edema [3].
- normal or enlarged ipsilateral epididymis. Reactive effusion with internal echoes is often detected [1].
- a spiral aspect of the cord or even a "Whirlpool sign" inside the sac or near the external inguinal ring [1].
 Fig 13: Partial testicular torsion in a 12-year-old boy who presented with acute testicular pain. a. Midline transverse image with B-flow technique reveals normal vascularity of both sides of the scrotum. b. Gray-scale longitudinal image demonstrates a slightly rounded left testis with normal echostructure and echogenicity in combination with a small hydrocele (asterisk). Left testis (LT). c. Split Color Doppler image demonstrates redundant spermatic cord (arrows) with normal vascularity on both sides of the scrotum. d. Color Doppler image of the left hemi-scrotum shows a tortuous appearance of the left spermatic cord (arrow) with preserved blow flow.
Fig 13: Partial testicular torsion in a 12-year-old boy who presented with acute testicular pain. a. Midline transverse image with B-flow technique reveals normal vascularity of both sides of the scrotum. b. Gray-scale longitudinal image demonstrates a slightly rounded left testis with normal echostructure and echogenicity in combination with a small hydrocele (asterisk). Left testis (LT). c. Split Color Doppler image demonstrates redundant spermatic cord (arrows) with normal vascularity on both sides of the scrotum. d. Color Doppler image of the left hemi-scrotum shows a tortuous appearance of the left spermatic cord (arrow) with preserved blow flow. Fig 14: Partial testicular torsion in a 15-year-old boy with 6 hours of acute right testicular pain. a. Gray-scale longitudinal image reveals a more spherical right testis with normal echostructure and echogenicity. A small hydrocele is also detected. Right testis (RT). b. Gray-scale longitudinal image reveals a normal left testis. Left testis (LT). c. Pulsed Doppler image shows a normal arterial waveform and RI index in the left testis. Left testis (LT). d. Pulsed Doppler image demonstrates an arterial waveform in the right testis, revealing decreased systolic flow compared to the contralateral testis, whereas the RI index is normal. Right testis (RT).
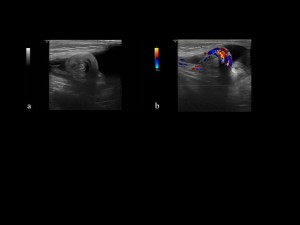
Fig 14: Partial testicular torsion in a 15-year-old boy with 6 hours of acute right testicular pain. a. Gray-scale longitudinal image reveals a more spherical right testis with normal echostructure and echogenicity. A small hydrocele is also detected. Right testis (RT). b. Gray-scale longitudinal image reveals a normal left testis. Left testis (LT). c. Pulsed Doppler image shows a normal arterial waveform and RI index in the left testis. Left testis (LT). d. Pulsed Doppler image demonstrates an arterial waveform in the right testis, revealing decreased systolic flow compared to the contralateral testis, whereas the RI index is normal. Right testis (RT). Fig 15: Partial testicular torsion in a 10-year-old boy with 8 hours of acute right testicular pain and nausea. a. Split gray-scale (longitudinal and transverse plane) image shows a normal left testis, measuring 6,81 cm3. b. Split gray-scale (longitudinal and transverse plane) image demonstrates an enlarged, rounded right testicle, also measuring 6,81 cm3. Fine hyperechogenic lines within the parenchyma indicate interstitial edema within testicular lobules. Free fluid is detected within the scrotal sac (arrow). c. Color Doppler imaging indicates spiral appearance (arrow) of the right spermatic cord with concentric arrangement of the vessels in the scrotal sac (Whirlpool sign).
Fig 15: Partial testicular torsion in a 10-year-old boy with 8 hours of acute right testicular pain and nausea. a. Split gray-scale (longitudinal and transverse plane) image shows a normal left testis, measuring 6,81 cm3. b. Split gray-scale (longitudinal and transverse plane) image demonstrates an enlarged, rounded right testicle, also measuring 6,81 cm3. Fine hyperechogenic lines within the parenchyma indicate interstitial edema within testicular lobules. Free fluid is detected within the scrotal sac (arrow). c. Color Doppler imaging indicates spiral appearance (arrow) of the right spermatic cord with concentric arrangement of the vessels in the scrotal sac (Whirlpool sign).
Color Doppler imaging reveals:
- usually preserved parenchymal blood flow [1]. The vascularity of the affected testis and epididymis can be normal or decreased. Furthermore, Color and Pulsed Doppler evaluation is critical primarily in cases with preserved parenchymal flow, since it can feature fine differences in the intratesticular vascular flow, the waveform of arterial flow, and the RI index between both sides of the scrotum. Pulsed Doppler may present with the following patterns [3]:Fig 13: Partial testicular torsion in a 12-year-old boy who presented with acute testicular pain. a. Midline transverse image with B-flow technique reveals normal vascularity of both sides of the scrotum. b. Gray-scale longitudinal image demonstrates a slightly rounded left testis with normal echostructure and echogenicity in combination with a small hydrocele (asterisk). Left testis (LT). c. Split Color Doppler image demonstrates redundant spermatic cord (arrows) with normal vascularity on both sides of the scrotum. d. Color Doppler image of the left hemi-scrotum shows a tortuous appearance of the left spermatic cord (arrow) with preserved blow flow.
- decreased systolic flow compared to the contralateral testis
- monophasic waveform of blood flow
- decreased diastolic flow velocities
- reverse diastolic flow
- increased RI index Fig 14: Partial testicular torsion in a 15-year-old boy with 6 hours of acute right testicular pain. a. Gray-scale longitudinal image reveals a more spherical right testis with normal echostructure and echogenicity. A small hydrocele is also detected. Right testis (RT). b. Gray-scale longitudinal image reveals a normal left testis. Left testis (LT). c. Pulsed Doppler image shows a normal arterial waveform and RI index in the left testis. Left testis (LT). d. Pulsed Doppler image demonstrates an arterial waveform in the right testis, revealing decreased systolic flow compared to the contralateral testis, whereas the RI index is normal. Right testis (RT).
- enlarged cord vessels with concentric arrangement within the torsion knot when blood flow is preserved. Fig 15: Partial testicular torsion in a 10-year-old boy with 8 hours of acute right testicular pain and nausea. a. Split gray-scale (longitudinal and transverse plane) image shows a normal left testis, measuring 6,81 cm3. b. Split gray-scale (longitudinal and transverse plane) image demonstrates an enlarged, rounded right testicle, also measuring 6,81 cm3. Fine hyperechogenic lines within the parenchyma indicate interstitial edema within testicular lobules. Free fluid is detected within the scrotal sac (arrow). c. Color Doppler imaging indicates spiral appearance (arrow) of the right spermatic cord with concentric arrangement of the vessels in the scrotal sac (Whirlpool sign).
Intermittent
Gray-scale imaging demonstrates:
- symmetric testicles in size, echostructure and echogenicity [1]. The affected testis can be in a horizontal or oblique lie.
- often a swollen ipsilateral epididymis along with reactive hydrocele.
- redundant spermatic cord in the scrotal sac [1].
 Fig 16: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 4 hours. a. Split gray-scale image shows longitudinal and transverse planes of the affected right testis, measuring longitudinal, transverse, and anteroposterior dimensions. Volume of the right testis: 14,44 cm3. b. Split gray-scale image shows longitudinal and transverse planes of the left testis, measuring three dimensions. Volume of the left testis: 14,6 cm3. The testes are almost symmetrical in size and have similar lie, echostructure and echogenicity. c. Split Color Doppler image reveals the epididymis of each side of the scrotum on a longitudinal plane. Both epididymis have normal size, lie, echostructure and vascularity. A small cyst in the head of the left epididymis (arrow) is recognized. Right epididymis (RT EPID), Left epididymis (LT EPID) d. Split Color Doppler interrogation of both testes indicates a slightly increased blood flow to the right testis, associated with detorsion as the pain was releaved.
Fig 16: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 4 hours. a. Split gray-scale image shows longitudinal and transverse planes of the affected right testis, measuring longitudinal, transverse, and anteroposterior dimensions. Volume of the right testis: 14,44 cm3. b. Split gray-scale image shows longitudinal and transverse planes of the left testis, measuring three dimensions. Volume of the left testis: 14,6 cm3. The testes are almost symmetrical in size and have similar lie, echostructure and echogenicity. c. Split Color Doppler image reveals the epididymis of each side of the scrotum on a longitudinal plane. Both epididymis have normal size, lie, echostructure and vascularity. A small cyst in the head of the left epididymis (arrow) is recognized. Right epididymis (RT EPID), Left epididymis (LT EPID) d. Split Color Doppler interrogation of both testes indicates a slightly increased blood flow to the right testis, associated with detorsion as the pain was releaved. Fig 17: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 5 days. The patient did not report any pain during the ultrasound exam. Surgery was performed for a Morgagni cyst, revealing bell clapper deformity bilaterally. a. Split Color Doppler imaging of both testicles shows a slightly increased intratesticular vascularity of the left testis. Right testis (RT), Left testis (LT). b. Split gray-scale and Color Doppler longitudinal plane indicates redundant and tortuous left spermatic cord (arrow) inside the scrotal sac with preserved blood flow. c. Split gray-scale longitudinal image shows reactive echogenic effusion (asterisk) in the scrotal sac. d. Gray-scale longitudinal plane reveals an anechoic lesion in the head of the epididymis measuring 1,44x0,77cm, which was palpable in the physical examination and pertains to a Morgagni cyst.
Fig 17: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 5 days. The patient did not report any pain during the ultrasound exam. Surgery was performed for a Morgagni cyst, revealing bell clapper deformity bilaterally. a. Split Color Doppler imaging of both testicles shows a slightly increased intratesticular vascularity of the left testis. Right testis (RT), Left testis (LT). b. Split gray-scale and Color Doppler longitudinal plane indicates redundant and tortuous left spermatic cord (arrow) inside the scrotal sac with preserved blood flow. c. Split gray-scale longitudinal image shows reactive echogenic effusion (asterisk) in the scrotal sac. d. Gray-scale longitudinal plane reveals an anechoic lesion in the head of the epididymis measuring 1,44x0,77cm, which was palpable in the physical examination and pertains to a Morgagni cyst.
Color Doppler imaging reveals:
- normal or potentially increased blood flow in cases of spontaneous detorsion of the affected testis [14]. Pulsed Doppler assessment reveals either a normal arterial flow waveform or waveform patterns, as described in partial torsion [3].
- a normal blood flow to the epididymis or increased in cases of spontaneous detorsion [14].
- preserved blood flow of the spermatic cord, or increased when detorsion is evident [14]. Fig 16: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 4 hours. a. Split gray-scale image shows longitudinal and transverse planes of the affected right testis, measuring longitudinal, transverse, and anteroposterior dimensions. Volume of the right testis: 14,44 cm3. b. Split gray-scale image shows longitudinal and transverse planes of the left testis, measuring three dimensions. Volume of the left testis: 14,6 cm3. The testes are almost symmetrical in size and have similar lie, echostructure and echogenicity. c. Split Color Doppler image reveals the epididymis of each side of the scrotum on a longitudinal plane. Both epididymis have normal size, lie, echostructure and vascularity. A small cyst in the head of the left epididymis (arrow) is recognized. Right epididymis (RT EPID), Left epididymis (LT EPID) d. Split Color Doppler interrogation of both testes indicates a slightly increased blood flow to the right testis, associated with detorsion as the pain was releaved.Fig 17: Intermittent testicular torsion in a 15-year-old boy who was admitted to the hospital for intermittent acute right testicular pain for the last 5 days. The patient did not report any pain during the ultrasound exam. Surgery was performed for a Morgagni cyst, revealing bell clapper deformity bilaterally. a. Split Color Doppler imaging of both testicles shows a slightly increased intratesticular vascularity of the left testis. Right testis (RT), Left testis (LT). b. Split gray-scale and Color Doppler longitudinal plane indicates redundant and tortuous left spermatic cord (arrow) inside the scrotal sac with preserved blood flow. c. Split gray-scale longitudinal image shows reactive echogenic effusion (asterisk) in the scrotal sac. d. Gray-scale longitudinal plane reveals an anechoic lesion in the head of the epididymis measuring 1,44x0,77cm, which was palpable in the physical examination and pertains to a Morgagni cyst.
In conclusion, Figure 18 summarizes all types of torsion.